About this pathway
Background
Ifosfamide (IF) is a widely used antitumor prodrug. It is in the oxazaphosphorine class of alkylating agents, and it is effective against solid tumors such as sarcomas and hematologic malignancies [Article:17464949]. Major clinical toxicities include urotoxicity, nephrotoxicity, encephalopathy and cardiotoxicity, as well as neurotoxicity (which occurs in approximately 20% of patients) [Article:22247713]. IF is used in combination chemotherapy, therefore drug-drug interactions are a possible source of increased toxicity as well as genetic variation or a combination of both [Article:12849722]. IF has lower myelotoxicity relative to its structural analog cyclophosphamide but higher rates (45% compared to 10%) of the nephrotoxic metabolite chloroacetaldehyde (CAA) [Article:21569511]. Variation in the renal expression of the P450 isozyme CYP2B6 is a factor responsible for tubular biotransformation of IF to its toxic metabolite CAA [Article:15875221] (discussed below). Glomerular and tubular dysfunctions represent serious side effects, especially in children who are co-treated with other nephrotoxic drugs. Thus, children are often supplemented with an equimolar dose of the organosulfur compound Mesna that prevents the build up of IF's toxic metabolites acrolein and CAA [Articles:10572607, 12849722].
Metabolism
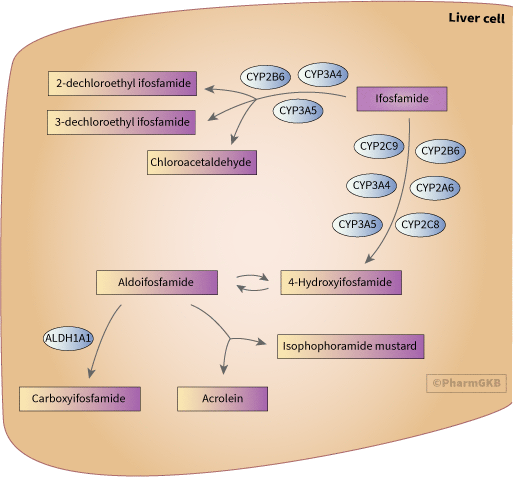
This diagram shows the genes involved in the biotransformation of IF and its metabolites, including pathways of activation, detoxification, and toxicity. The metabolism of IF is parallel to that of cyclophosphamide but with some differences in isozyme specificities and reaction kinetics [Articles:18781911, 16393888].
Activation of IF to 4-hydroxyifosfamide is catalyzed by the hepatic cytochrome P450 (CYP) isoforms CYP3A4 and 2B6 with 2A6, 2C8, 2C9 and 2C19 making more minor contributions [Articles:16393888, 17464949]. Although IF requires CYP3A4 and CYP2B6 for bioactivation and metabolism, CYP3A4 is mainly responsible for the transformation of IF to active product via auto induction. IF auto induces it's own biotransformation by activating the xenobiotic receptor PXR coded by NR1I2 which mediates autoinduction by transcriptional upregulation of CYP3A4 [Article:21487929]. IF's ability to auto induce suggests its drug metabolism may increase over time. Contrary to cyclophosphamide and other drugs, IF's metabolism by CYP3A4 leads to more toxic metabolites [Article:17464949].
Competing with, and split about evenly with 4-hydroxylation, is a major oxidative detoxification pathway that results in both the detoxified 2- or 3-dechloroethylifosfamide (DCE) and the formation of CAA (toxic), both primarily mediated by CYP2B6 and CYP3A4 in the liver [Articles:17464949, 18781911]. 4-Hydroxyifosfamide rapidly interconverts with its tautomer, aldoifosfamide. It is likely that both of these metabolites passively diffuse out of hepatic cells, circulate, and then passively enter other cells [Article:1922424]. Aldoifosfamide partitions between ALDH1A1-mediated detoxification to the inactive metabolite carboxyifosfamide and a spontaneous (non-enzymatic) elimination reaction to yield the therapeutically active metabolite isophosphoramide mustard (IPM) and acrolein (associated with bladder toxicity) [Article:16393888]. IPM, the DNA crosslinking agent of clinical significance, is a circulating metabolite but the anionic IPM does not enter cells as readily as its metabolic precursors [Article:18028906] (not depicted here, see the ifosfamide pharmacodynamics pathway for details)
Like cyclophosphamide, IF is chiral at phosphorus but unlike the case for cyclophosphamide, enantioselectivity in IF metabolism may have clinical significance. This is particularly relevant to the distribution of 4-hydroxylation versus N-dechloroethylation products and the impact of this on the CNS toxicity associated with IF therapy. The differences in the metabolism and disposition of the R- and S-enantiomers of IF have not been fully evaluated in human tissues. Nevertheless, in several studies using characterized human liver microsomes or cDNA-expressed isozymes it has been shown that ®-IF is subject to less dechloroethylation, a more rapid 4-hydroxylation, and increased toxicity relative to the (S)-IF [Article:17855037].
Toxicity
High rates of toxicity in kidney cells are evident following IF treatment. The kidney is capable of metabolizing IF through its abundance of xenobiotic metabolizing enzymes [Article:15875221]. Metabolism in the kidney and liver may differ based on the relative abundance of CYP isotypes specifically CYP2B6, CYP3A4, CYP3A5. Furthermore, genetic variance of these CYPs in the liver can be influenced by sex. Generally, there are two fold higher levels of CYP3A4 protein in females than in males but overall variation of CYP3A4 in the liver is up to 100 fold. There are fairly undetectable levels of the CYP2B6 protein in pediatric livers. The allele CYP2B6*6 results in 50-75% lower liver protein expression. In the kidney there are low levels of CYP2B6 mRNA transcripts but CYP3A5 protein expression is predominant. Renal biotransformation in the kidney can be quicker than in liver cells and this is based on variation and abundance of the CYP2B6, 3A4, 3A5 isotypes. It is estimated the variability of these CYPs range from 40-400 fold [Articles:23333322, 17465708]. CYP3A4 and CYP3A5 are present in the kidney prior to birth so this pathway route is likely active early on. Children three years of age and younger suffer serious renal damage and so in pediatric cases patients are coadministered Mesna, a uroprotective agent, which can prevent the toxic metabolites acrolein and CAA that typically lead to hemorrhagic cystitis [Articles:23220588, 12849722, 10572607]. (Refer to the ifosfamide pharmacodynamics pathway for mechanisms of the toxic metabolites acrolein and CAA).
Pharmacogenomics
Large interpatient differences, which may be up to 20-fold, in the pharmacokinetics and biotransformation of IF have been reported [Article:18781911].
CYP2B6 allele CYP2B6*6 heterozygous and homozygous carriers has been linked with lower catalytic activity and protein expression in the liver, higher concentrations of IF in plasma, and higher rates of CAA associated toxicity. Oppositely, allele CYP2B6*1 has been shown to have higher catalytic activity, higher protein expression, and a higher rate of clearance of IF [Article:18781911]. In addition, alike to CYP2B6*6, 14-25% of CYP2B6*5 Caucasian female carriers display lower protein expression and catalytic activity in the liver resulting in lower rates of clearance and higher amounts of CAA [Article:18781911].
Carriers of CYP3A5*1 have shown to catalyze the detoxification pathway to DCE at a faster rate leading to a greater amount of CAA and higher risk of nephrotoxicity due to CAA's ability to rapidly degrade in human blood [Article:15821045].
Conclusions
With cancer drugs it is often difficult to reduce toxicity because metabolism of the drug in the liver and kidney is necessary for release of the active component, and toxic metabolites can be required for efficacy. Knowledge of the relative production of toxic metabolites at different sites and how this is influenced by genotype could be useful. Further insight regarding P450 CYP haplotype variation and the resulting phenotypes would be beneficial and contribute to a more comprehensive understanding of the kinetics pathway. In addition, it would be advantageous to look at more adjuvants to suppress the toxic byproducts of IF.
Reactions & interactions (16)
-
Biochemical Reaction
ifosfamide → 3-dechloroethyl ifosfamide + chloroacetaldehyde
-
Biochemical Reaction
ifosfamide → 2-dechloroethyl ifosfamide + chloroacetaldehyde
-
Biochemical Reaction
4-hydroxyifosfamide → aldoifosfamide
-
Biochemical Reaction
aldoifosfamide → carboxyifosfamide
-
Biochemical Reaction
ifosfamide → 4-hydroxyifosfamide
-
Biochemical Reaction
aldoifosfamide → acrolein + isophosphoramide mustard
-
Catalysis
CYP3A4 → Biochemical Reaction
-
Catalysis
CYP3A5 → Biochemical Reaction
-
Catalysis
CYP2B6 → Biochemical Reaction
-
Catalysis
ALDH1A1 → Biochemical Reaction
-
Catalysis
CYP2C9 → Biochemical Reaction
-
Catalysis
CYP2A6 → Biochemical Reaction
-
Catalysis
CYP2B6 → Biochemical Reaction
-
Catalysis
CYP3A5 → Biochemical Reaction
-
Catalysis
CYP2C8 → Biochemical Reaction
-
Catalysis
CYP3A4 → Biochemical Reaction
Edit history (4)
- 2005-01-18 Create
- 2013-03-26 Update
- 2019-02-13 Update Updated to new illustrator formatting.
- 2019-02-14 Update Updated gpml to new format.