About this pathway
The renin-angiotensin-aldosterone system (RAAS) is central to the control of blood pressure and the target of several types of anti-hypertensive drugs. This pathway depicts a simplified representation of the pharmacodynamics (PD) of RAAS-acting drugs including candidate genes for the pharmacogenomics (PGx) of ACE inhibitors, angiotensin receptor blockers (ARBs), renin inhibitor aliskiren and aldosterone receptor antagonists.
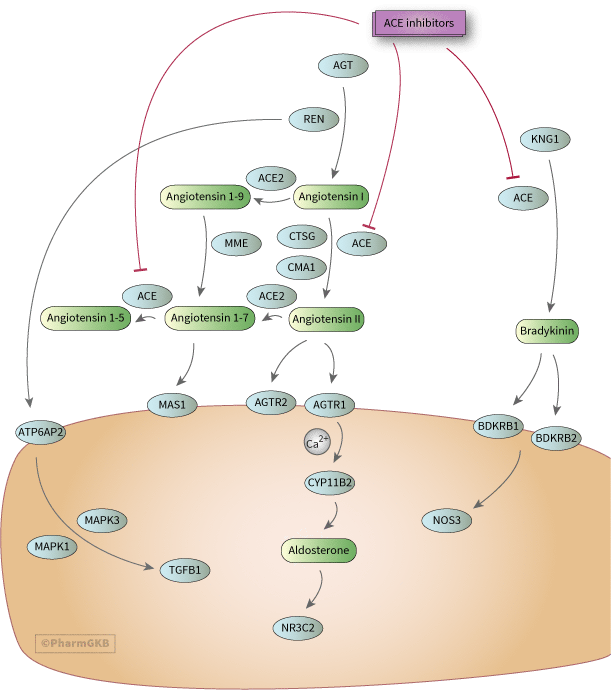
The core of this pathway was elucidated over a century ago and involves the conversion of angiotensinogen to angiotensin I (Ang I) by renin, its subsequent conversion to angiotensin II (Ang II) by angiotensin converting enzyme. Ang II activates the angiotensin II receptor type 1 to induce aldosterone synthesis, increasing water and salt resorption and potassium excretion in the kidney and increasing blood pressure [Article:18035185]. The key candidate genes involved in the core pathway are angiotensinogen, AGT; renin, REN; angiotensin converting enzyme, ACE; and angiotensin II receptor type 1, AGTR1.
Although depicted in the center of the pathway in this graphic, the ACE gene product, angiotensin converting enzyme, is predominantly found attached to the plasma membrane (tissue bound ACE). ACE can be released into plasma (soluble ACE); however this form is not considered to catalyze the cleavage of Ang I to Ang II [Articles:9153279, 1510141] ACE inhibitor class of drugs on candidate genes in the renin-angiotensin-aldosterone pathway (RAAS). ACE inhibitors target the ACE gene product resulting in downstream reduction of Ang II, decreasing aldosterone secretion and reducing blood pressure. ARBs target AGTR1 blocking its activation, also resulting in lower levels of aldosterone and lower blood pressure. The decrease in aldosterone decreases sodium and water resorption, decreases potassium excretion and decreases blood pressure. Angiotensin signaling downstream of AGTR1 can occur through several different pathways, including modulation of intracellular calcium, but also via 12-lipoxygenase, PKC and src kinase family routes (not depicted in detail) [Article:15134803]. The type 2 angiotensin receptor, AGTR2, is considered to act in opposition to AGTR1, inducing vasodilation, growth inhibition and apoptosis [Article:18035185]. ARBs are selective for AGTR1 and do not bind to AGTR2. The story with both angiotensin receptors is a good deal more complex than pictured as recently several GPCR interacting proteins have been identified that modulate both receptor actions as well as receptor dimerization and activation without ligands by mechanical forces [Article:17717300]. Activation of AGTR1 and downstream signaling including release of calcium leads to transcriptional upregulation of CYP11B2, aldosterone synthase, and synthesis of aldosterone from cholesterol [Article:15134803]. The mineralocorticoid receptor, NR3C2, to which aldosterone binds, is the target for spironolactone and eplerenone [Articles:15134803, 18729003].
The suppression of aldosterone by ACE inhibitors is incomplete since alternative pathways can still generate Ang II via chymase (CMA1) or cathepsin G (CTSG) degradation of Ang I [Article:18035185]. This is known as aldosterone escape or breakthrough. It has also been observed with ARBs [Article:17376010]. Aliskiren, acting upstream of ACE, is thought to avoid this, however the discovery of the Pro-renin and renin receptor ((P)RR, coded for by ATP6AP2) is very recent and its role in the pathway not yet understood [Article:18417113]. In order to achieve sufficient decrease in blood pressure, patients often receive multiple drugs, and poly-therapy is the norm in secondary cardiovascular event prevention, heart failure and diabetes. Through their action on the bradykinin pathway, ACE inhibitors also increase production of nitric oxide and induce vasodilation through this route [Articles:18182246, 9207629]. ACE2, its products and their receptor MAS1 represent relatively recent additions to the candidate genes for this pathway [Article:18449520]. Thus the RAAS is not the simple endocrine system as was initially thought.
There is considerable inter-individual variation in response to antihypertensive treatments. PGx offers the potential to achieve better blood pressure control in hypertensive patients, prevent organ damage in cardiovascular and renal diseases and reduce side effects. Adverse drug responses (ADRs) to ACE inhibitors include mild side effects such as cough and serious side effects such as angioedema [Article:16679330]. ARBs have fewer reported side effects; however, the long term benefits are still not as clear as those of ACE inhibitors [Article:16679330]. Aliskiren is also reported to have a favorable side effect profile [Article:17956203], although recently a case of drug-induced long QT syndrome and torsades de pointes was reported [Article:19279548]. Side effects of spironolactone and eplerenone are hyperkalemia (both) and gynecomastia (spironolactone only) [Article:18729003].
PGx studies of antihypertensive PD have examined genes in the RAAS pathway with the insertion/deletion (I/D) polymorphism in ACE being the most commonly studied variant [Article:15174896] and ACE inhibitors the most studied drugs. The I/D polymorphism has been variously reported in the literature as rs1799752, rs4646994, rs4340, and rs13447447 (although the latter rs numbers have been retired as of 2016). More details including mapping information can be found in the ACE VIP annotation. In the majority of PGx studies of ACE inhibitors, the D allele has tended to be associated with greater lowering of blood pressure, but the results are inconclusive [Articles:19074621, 19497121]. PGx studies of ACE I/D and other RAAS-acting drugs also have had mixed results [Article:15174896]. Since coughing is not a side effect of ARBs or renin inhibitors, it is considered to be related to the bradykinin pathway actions of ACE inhibition [Article:8583482] and a BDKR2 polymorphism has been associated with ACE inhibitor-induced cough [Articles:12522467, 10904024].
The PERGENE study recently reported an association of a bradykinin receptor SNP with response to ACE inhibitors in Europeans with stable coronary artery disease. BDKRB1 rs12050217 AA homozygotes had reduced HR for cardiac events while treated with perindopril (n = 8907)[Article:20712529].
The rs5182 C allele in AGTR1 (573C>T) was associated with reduced risk of myocardial infarction in ACE inhibitor users with hypertension (n= 4097)[Article:18347611]. However, recent results from the PERGENE study showed reduced risk cardiac events for TT homozygotes with stable coronary artery disease (n = 8907)[Article:20712529]. The PERGENE study also associated homozygotes for the common allele of rs275651 (TT) with reduced risk for cardiac events (n = 8907)[Article:20712529]. Polymorphisms in AGT (AGT:Met235Thr, rs699) and AGTR1 (AGTR1:1166A>C, rs5186) have also been examined in studies of RAAS-acting drugs, but with conflicting results (see variant annotations). A recent study identified a variant in NOS3 (NOS3(-786)T>C, rs2070744) as associated with treatment-resistant hypertension, where treatment was up to three antihypertensive drugs and included ACE inhibitors and ARBs as well as diuretics, beta and alpha blockers and calcium channel blockers [Article:19650939]. To date, there are no reports catalogued in PubMed that looked at the pharmacogenomics of aliskiren.
Although currently there are no treatment guidelines for RAAS-acting drugs based on genomics, large multi-gene haplotype and Genome Wide PGx studies such as PERGENE may provide clearer evidence to improve therapeutic choices, reduce side effects, improve blood pressure control and prevent organ damage.
Reactions & interactions (35)
-
Activation
ATP6AP2 → MAPK1
-
Activation
angiotensin II → AGTR2
-
Activation
REN → ATP6AP2
-
Activation
angiotensin 1-7 → MAS1
-
Activation
MAPK3 → TGFB1
-
Activation
ATP6AP2 → MAPK3
-
Activation
angiotensin II → AGTR1
-
Activation
MAPK1 → TGFB1
-
Activation
BDKRB2 → NOS3
-
Activation
bradykinin → BDKRB2
-
Activation
bradykinin → BDKRB1
-
Activation
aldosterone → NR3C2
-
Activation
AGTR1 → CYP11B2
-
Activation
calcium → CYP11B2
-
Activation
AGTR1 → calcium
-
Biochemical Reaction
angiotensin I → angiotensin II
-
Biochemical Reaction
angiotensin 1-9 → angiotensin 1-7
-
Biochemical Reaction
AGT → angiotensin I
-
Biochemical Reaction
angiotensin 1-7 → angiotensin 1-5
-
Biochemical Reaction
angiotensin I → angiotensin 1-9
-
Biochemical Reaction
angiotensin II → angiotensin 1-7
-
Biochemical Reaction
KNG1 → bradykinin
-
Biochemical Reaction
CYP11B2 → aldosterone
-
Catalysis
CTSG → Biochemical Reaction
-
Catalysis
CMA1 → Biochemical Reaction
-
Catalysis
ACE → Biochemical Reaction
-
Catalysis
MME → Biochemical Reaction
-
Catalysis
REN → Biochemical Reaction
-
Catalysis
ACE → Biochemical Reaction
-
Catalysis
ACE2 → Biochemical Reaction
-
Catalysis
ACE2 → Biochemical Reaction
-
Catalysis
ACE → Biochemical Reaction
-
Inhibition
Ace Inhibitors, Plain → ACE
-
Inhibition
Ace Inhibitors, Plain → ACE
-
Inhibition
Ace Inhibitors, Plain → ACE
Edit history (6)
- 2005-12-01 Create
- 2012-02-07 Update
- 2016-11-07 Note Noted retired rs# for the insertion/deletion variant.
- 2019-03-28 Update Updated to new illustrator formatting.
- 2019-06-18 Update Updated to new gpml format.
- 2025-06-19 Update fixed typos