About this pathway
Introduction
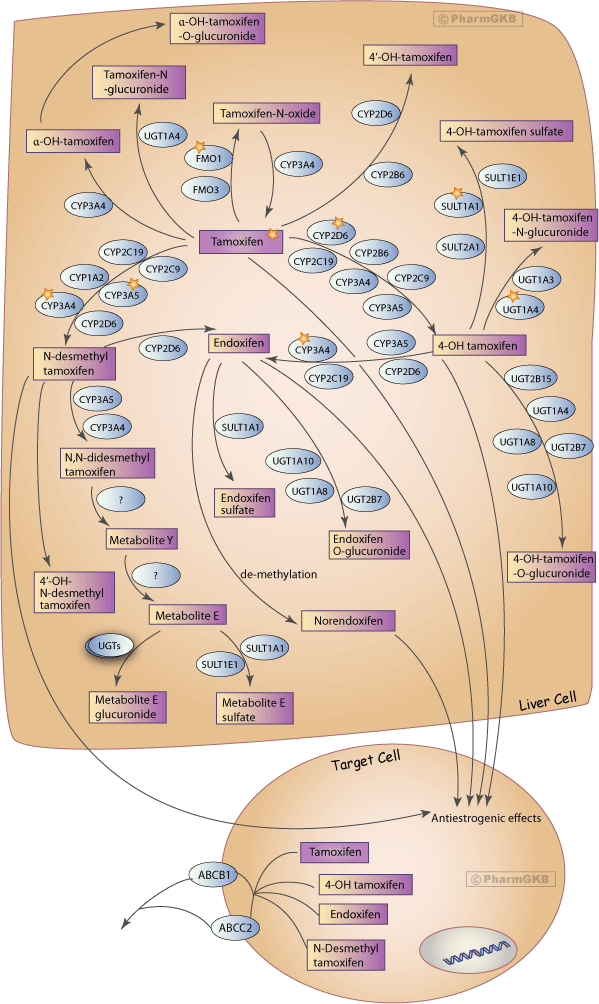
Tamoxifen, a selective estrogen receptor modulator (SERM), is important for the treatment and prevention of estrogen receptor (ER) positive breast cancer. It has been shown to decrease disease recurrence and mortality rates by as much as 50% and 30% respectively, and has also been used as a prophylactic treatment for those at high risk of developing breast cancer [Articles:9747868, 11023543, 15159443, 16361630, 18024866, 21961651]. The response to tamoxifen has a high degree of inter-individual variability, the cause of which may be due, in part, to differences in its metabolism in vivo [Article:15159443] (Figure 1). Hot flashes, the most common side effect of tamoxifen, affect up to 80% of women [Articles:14652227, 14652237, 18829880]. Patients receiving tamoxifen also seem to have approximately 2.5 times higher risk of developing endometrial cancer [Articles:2563046, 9747868, 9828250]. Additionally, tamoxifen may contribute to an increased risk for thromboembolic events as well as clinical depression [Articles:9747868, 18829880]. Selective serotonin reuptake inhibitors (SSRIs) are commonly used to treat both hot flashes and depression, but clinicians need to choose carefully when deciding which SSRI to prescribe since many may have the capacity to decrease the efficacy of tamoxifen treatment [Articles:14652237, 15632378, 17115111, 17245346, 18829880].
Tamoxifen is used as an ER antagonist, which competitively inhibits cancerous ER positive cells from getting the estrogen required for growth [Articles:165942, 170527, 9828250]. However, it has long been thought that tamoxifen is actually a prodrug, and that its metabolites are likely to be the causative factors for the success seen in tamoxifen therapy [Articles:591813, 7470748]. For more information on the seminal works regarding tamoxifen, please see this excellent review by Jordan [Article:12612646]. Besides acting as SERMs, it has recently been found that some of tamoxifen's metabolites also act as aromatase inhibitors in vitro [Articles:21390495, 21814747]. Aromatase converts steroids (e.g., testosterone to estradiol), the inhibition of which severely decreases the amount of available estrogen in the body. A previously unrecognized metabolite of tamoxifen, norendoxifen, is the most potent aromatase inhibitor of the tamoxifen metabolites. It caused the same decrease in vitro in aromatase activity as letrozole, a drug that is exclusively marketed as an aromatase inhibitor [Article:21814747].
This pathway summary illustrates many of the genes involved in the complex network of tamoxifen metabolism and provides a brief overview of why variation in those genes may perturb the balance of the different tamoxifen metabolites and result in different drug response outcomes.
Pharmacokinetics
Tamoxifen is extensively metabolized predominantly by the cytochrome P450 (CYP) system to several primary and secondary metabolites, some of which exhibit more antiestrogenic effects in breast cancer cells than tamoxifen itself [Articles:15159443, 21451508, 22041137]. Tamoxifen metabolism mostly occurs via two pathways, 4-hydroxylation and N-demethylation, both of which result in the very potent secondary metabolite, endoxifen. Originally, the 4-hydroxylation path, which is catalyzed by multiple CYPs including CYP2D6, was given much attention because the immediately resulting metabolite, 4-hydroxy-tamoxifen, had been shown to be approximately 30- to 100-fold more potent as an antiestrogen than tamoxifen [Articles:591813, 15159443]. However, this pathway only contributes approximately 7% of tamoxifen metabolism. N-demethylation to N-desmethyltamoxifen, catalyzed primarily by CYP3A4 and CYP3A5, contributes approximately 92% of tamoxifen metabolism [Articles:14652237, 15159443, 22041137]. N-desmethyltamoxifen is further oxidized to a number of metabolites that appear important to tamoxifen activity, the most important being endoxifen. Endoxifen, first identified in human bile [Article:3349495], is formed from N-desmethyltamoxifen through hydroxylation by CYP2D6, and from 4-hydroxy-tamoxifen through demethylation by CYP3A4 [Articles:14652237, 22041137]. While 4-hydroxytamoxifen and endoxifen have similar potencies in terms of antiestrogenic activity, endoxifen plasma concentrations in those receiving tamoxifen therapy is, on average, over ten-fold higher than that of 4-hydroxytamoxifen with large interpatient variability [Articles:14652237, 16815318, 21961651, 21451508]. In addition to the estrogen receptor inhibition exhibited by endoxifen, it also uniquely targets ERα (coded for by ESR1 gene) for proteasomal degradation. Endoxifen alone causes a decrease in ERα protein levels while the other metabolites of tamoxifen merely stabilize them. Because of this added effect, endoxifen is likely to be the primary metabolite responsible for the success seen in tamoxifen treatment [Article:19244106].
Tamoxifen is also metabolized by the flavin monooxygenases FMO1 and FMO3 to form tamoxifen-N-oxide (TNO). This can then be reduced back to tamoxifen in vitro by multiple cytochrome P450's, the most prominent in terms of velocity of reduction being CYP1A1, CYP2A6, and CYP3A4. Also, it should be noted that only reduction of TNO by CYP3A4 produced tamoxifen that was further metabolized. However, it has been shown that TNO can be reduced to tamoxifen by hemoglobin and NADPH-P450 oxidoreductase. This yields the possibility that the reduction of TNO is not enzymatically dependent, but may be accomplished by the heme-iron complex that hemoglobin and the cytochromes have in common. This suggests that an in vivo cycle may exist that uses TNO as a storage unit for tamoxifen [Article:15987777]. In accordance with this possibility, it has been shown that the ratio of tissue to serum concentration of TNO decreases with increasing doses of tamoxifen while the tissue to serum concentration ratios of tamoxifen and its other metabolites remain constant. This is likely due to a quick reduction of TNO to tamoxifen in tumor cells where the anticancer activity of tamoxifen is most needed [Article:22562123]. While these observations are interesting, the likelihood that TNO may be chemically reduced during sample preparation cannot be excluded, which makes it currently difficult to determine the precise role of TNO in the overall metabolism and effect of tamoxifen.
While breast tissue does not usually express the multidrug resistance gene 1/ATP-binding cassette B1 (MDR1/ABCB1), some tumors do express this gene. Breast cancer can metastasize to the brain, behind the blood brain barrier, where ABCB1 is also expressed. Since tamoxifen and its metabolites, particularly endoxifen, are substrates of P-glycoprotein, ABCB1 may keep cellular concentrations of tamoxifen and its metabolites low, at subtherapeutic levels. At high doses, tamoxifen is used to treat tumors that have metastasized to the brain. It is likely that at the doses used in these settings, drug transporters in the blood brain barrier may be already saturated and may not prevent tamoxifen and metabolites to access the brain [Articles:21378205, 21148080].
Tamoxifen and its metabolites are inactivated via glucuronidation and sulfation through various UGTs and SULTs, respectively [Articles:16381672, 20565970]. Glucuronidation is the more prominent pathway; approximately 75% of the tamoxifen dose is excreted into the biliary tract as glucuronides [Article:20124171]. Most of the human UGTs exhibit some activity with tamoxifen or its metabolites while sulfation is mainly accomplished by SULT1A1 [Articles:12419790, 16381672, 17664247, 22041137].
Pharmacogenomics
Given the preponderance of enzymes that participate in tamoxifen metabolism, there are many gene variants that may affect the relative amounts of the different tamoxifen metabolites. The CYP450 enzymes are highly polymorphic with many well-characterized variants, as are the UGT and SULT genes.
CYP2D6
Observational studies examining the treatment of tamoxifen side effects with SSRIs first pointed to the role of CYP2D6 as a modulator of efficacy [Article:14652237]. During the past ten years, more than 20 published studies have examined the role of CYP2D6 genotype in tamoxifen treatment outcome [Article:22531359]. There is still much debate about its clinical relevance [Article:23091108].
The majority of studies of tamoxifen pharmacogenomics have been candidate gene based and have examined the role of the CYP2D6 gene (/gene/PA128?tabType=tabVip). CYP2D6 has variants that can result in enzymes that correlate to a wide range of metabolic activity. There are four phenotypic categories to which patients can be assigned based on their CYP2D6 enzymatic function: poor metabolizers (PM) have enzymes with no activity, intermediate metabolizers (IM) have reduced functional enzymes, extensive metabolizers (EM) have enzymes with normal function, and ultra-rapid metabolizers (UM) have enzymes with above average enzyme function [Article:19512959].
Because CYP2D6 is responsible for the hydroxylation of N-desmethyltamoxifen to endoxifen, genetic variations that cause differences in CYP2D6 metabolizer status may play a role in individual therapeutic benefit. This has led to research into the possible association between CYP2D6 genotype and maximum benefit from tamoxifen therapy. Some research suggests that CYP2D6 PMs have worse prognoses than those with typical enzyme activity [Articles:14652227, 16361630, 16877740, 16815318, 17115111, 17761971, 18024866, 17245346, 19809024, 19244106, 20124171, 21378205] though contradictory evidence does exist [Articles:15952058, 15987423, 17244352]. Specifically, two large studies have recently been published providing evidence against this association and asserting that CYP2D6 genotyping prior to treatment serves no clinical benefit [Articles:22395643, 22395644]. These two studies have been the subject of intense discussion among scientists in this field [Articles:22851270, 22851267, 23091108]. There are a number of reasons that these differences in outcomes may be seen. The International Tamoxifen Pharmacogenomics Consortium (ITPC) is in the process of publishing a manuscript detailing the difficulties of reaching consensus in regards to CYP2D6 genotype as a predictor for tamoxifen response . Principal among these difficulties may be accurately genotyping and phenotyping CYP2D6. Copy number is not always assessed, which may cause for a misclassification of metabolizer status. CYP2D6 also has pseudogenes that alter enzymatic activity and are hard to detect. For example, upon further inspection of CYP2D6*4, one of the more common non-functional alleles, one study found that 18.7% of the CYP2D6*4 alleles were actually CYP2D6-2D7 hybrid alleles [Article:22676198]. Environmental factors, such as menopausal status or potential drug interactions with CYP2D6 inhibitors like SSRIs, are also not always considered, but can cause a big change in phenotype [Article:23091108].
Other candidate pharmacogenes
The CYP2C19*17 higher functioning variant has been associated with better responses to treatment, lower adverse reactions, and increased disease free survival [Articles:18024866, 20565970]. Due to the increased metabolism exhibited by the *17 allele, tamoxifen may be converted more efficiently to its more active metabolites. Patients with the *17 allele also seem to be at a decreased risk for developing breast cancer in general [Articles:18521743, 20565970]. This may be due to the increased metabolism of, and thus decreased levels of, endogenous estrogens [Articles:18521743, 20565970]. The lower levels of endogenous estrogens may also explain why patients with the *17 allele seem to respond better to treatment with tamoxifen. If the body decreases the amount of available estrogen prior to treatment, the continued decrease of exposure to estrogen resulting from treatment should result in better patient outcome. However, the association with the *17 allele and increased disease free survival has not been shown in all studies [Article:21961651].
SULT1A1 is the most prominent gene involved in sulfation and has two major alleles, SULT1A1*1 and SULT1A1*2. SULT1A1*1, the higher functioning allele, is associated with better patient survival as compared to SULT1A1*2 [Articles:12419790, 15952058, 17244352]. SULT1A1 copy number, which has also been shown to affect enzyme activity, seems to have no effect on survival [Article:21961651]. Variants in UGT2B15, known for metabolizing steroids as well as xenobiotics, have also been shown to affect survival and disease recurrence. UGT2B15*2, the higher functioning variant, has been associated with decreased overall survival and increased disease recurrence. This association is much stronger when both SULT1A1 and UGT2B15 genotypes are evaluated together [Article:15952058].
Two single nucleotide polymorphisms (SNPs) outside of the CYP450s have been associated with clinical outcomes of tamoxifen therapy. A genome wide association study (GWAS) in a Japanese population revealed that rs10509373 in chromosome 10 open reading frame 11 (C10orf11) at the 10q22 locus is associated with an increased recurrence free survival, though this SNP is in an intronic region and may not be directly responsible for this association. It is located within a 172-kb linkage disequilibrium block including the C10orf11 gene, and thus the causative SNP may be contained within that region [Article:22180457]. rs3740065, located in ABCC2, is associated with increased expression of ABCC2, which may lead to lower exposure of breast tissue to the active metabolites and is associated with decreased disease-survival time [Article:20124171].
Conclusion
The clinical importance of CYP2D6 genotype to treatment outcome has yet to be fully determined. Nonetheless, tamoxifen continues to be widely and relatively successfully used to treat ER positive breast cancer. Although the cumulative research has been unable to completely explain the high degree of interindividual variability, reasons for the contradictory evidence are currently emerging and should be implemented in the study design of future research. Specifically, as evidenced by the lack of a known therapeutic concentration, studies relating in vivo concentrations of tamoxifen metabolites to clinical outcomes are scant. Thus, it will be necessary to examine network effects across variants in all pathway genes. Study cohorts with clearly defined and tightly controlled phenotypes (menopausal status, indication, dose and duration, co-treatments, outcomes and follow-up) and strict genotypes/metabolizer status groupings may cut down confounding issues.
Edit history (5)
- 2005-08-25 Create
- 2011-08-04 Update
- 2012-06-26 Update
- 2013-05-02 Update
- 2013-09-28 Update