About this pathway
Introduction
Doxepin is a tricyclic antidepressant (TCA). It is approved for the use in treatment of major depression and insomnia [Article:22681161]. Doxepin is also utilized as part of the treatment of chronic urticaria [Article:9111875] and in pain management [Articles:19724772, 8638990].
Doxepin is shown to inhibit the reuptake of noradrenalin and serotonin. The reuptake inhibition of dopamine is very weak. Doxepin's metabolite desmethyldoxepin (nordoxepin) also has antidepressant effects.
Doxepin binds strongly to the histamine H1 and H2 receptors [Article:22701403]. Its selective histamine antagonist function is responsible for the drug's sleep-promoting properties [Article:17685877]. Doxepin also acts antagonistic on 5-hydroxytryptamine (serotonin) receptors, alpha 1 adrenergic receptors and muscarinic cholinergic receptors [Article:17685877]. The crystal structure of the H1R complex together with doxepin was solved recently [Article:21697825].
Pharmacokinetics
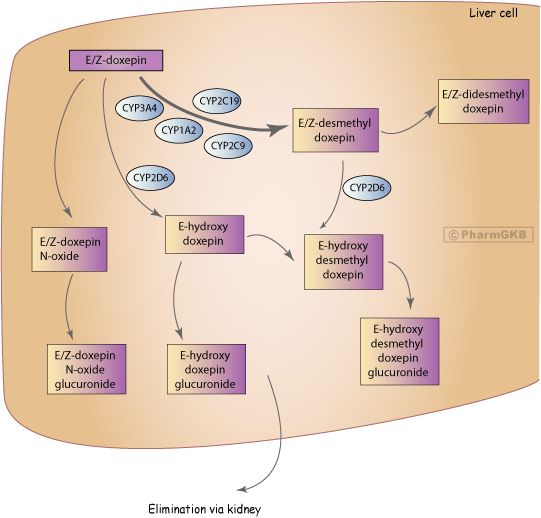
Conventional doxepin preparations are a mixture of Z (cis)- and E (trans)-isomers in a ratio 15:85 [Article:1607001]. The E-isomer is more active as a serotonin reuptake inhibitor, while the Z-isomer shows greater activity as a sedative. The major route of metabolism of both isomers of doxepin is demethylation to the active metabolite desmethyldoxepin. This is carried out by the cytochrome P450 2C19 (CYP2C19) with a possible minor involvement of CYP1A2, CYP3A4 or CYP2C9 [Articles:12360109, 12180536, 11037801]. Hydroxylation of doxepin by CYP2D6 is mostly specific to the E-isomer. Desmethyldoxepin is also hydroxylated by CYP2D6 [Articles:12360109, 16007002, 11037801]. The hydroxylated isomers are glucuronidated [Articles:1981729, 9733660]. Another pathway is oxidation to doxepin N-oxide, which is also then glucuronidated [Article:1981729]. The ratio between Z- and E desmethyldoxepin is around 50:50 [Article:1981729]. Didesmethyldoxepin, the demethylated product of desmethyldoxepin, was found in patients' plasma and cerebrospinal fluid [Article:9181631].
The plasma protein binding of doxepin and desmethyldoxepin is about 80% [Articles:7113722, 7293791]. Unbound to plasma protein, doxepin is lipophilic and can pass easily through the blood-brain-barrier. A close correlation between cerebrospinal fluid and plasma concentrations is seen for both doxepin and desmethyldoxepin, which suggests that the blood-brain-barrier is constantly permeable to doxepin and desmethyldoxepin [Article:21350940].
Pharmacogenetics
Variability of doxepin plasma concentration might contribute to interindividual differences in treatment response and side effect severity. An optimal range of plasma concentration of TCA that correlates well to treatment response has been defined based on therapeutic drug monitoring [Article:22053351]. The therapeutic reference range/recommended drug concentration for doxepin plus desmethyldoxepin is 50-150 ng/mL [Article:22053351].
CYP2D6 and CYP2C19 enzymes are encoded by highly polymorphic genes, which might affect the metabolism of doxepin resulting in sub-therapeutic plasma concentration of doxepin and its metabolites, causing treatment failure or increased risk of side effects.
Table 1 summarizes the effect of CYP2D6 and CYP2C19 metabolizer phenotypes on the pharmacokinetics of doxepin.
Subjects with the CYP2D6 poor metabolizer (PM) phenotype might have reduced clearance of doxepin and desmethyldoxepin, which results in a higher plasma concentrations compared to subjects with the CYP2D6 extensive metabolizer (EM) phenotype as shown by two small studies in healthy volunteers exposed to a single dose of 75 mg doxepin [Articles:12360109, 16007002]. In one of the above studies, CYP2D6 ultrarapid metabolizers (UM) showed an increased clearance and lower doxepin and nordoxepin plasma concentration [Article:16007002]. In addition, a case report identified a CYP2D6 PM involved in a fatal doxepin poisoning due to blood concentration of doxepin 16-80 times higher than therapeutic concentrations [Article:17721180]. Larger studies investigating the association of CYP2D6 variants and clinical outcome (treatment response and/or side effects) of doxepin therapy are needed to extend previous findings.
Currently only one small-sized study has investigated the effect of genetic variations in the CYP2C19 gene on doxepin metabolism. This used a single dose of doxepin in healthy volunteers [Article:12360109]. The median oral clearance of doxepin (Z-doxepin) differed 2-fold between CYP2C19 EMs and PMs, but desmethyldoxepin was detected in CYP2C19 PMs reflecting the involvement of additional cytochrome P450 enzymes in demethylation step (Figure1). Further studies are necessary to clarify the impact of CYP2C19 polymorphisms on doxepin response and side effects.
The Royal Dutch Pharmacists Association - Pharmacogenetics Working Group [Article:21412232] and the Clinical Pharmacogenetics Implementation Consortium (CPIC®) [Article:27997040] have published clinical prescribing guidelines for doxepin. Both include recommendations for all non-CYP2D6 Normal metabolizer phenotypes, which are summarized in the Clinical Guideline Annotations section.
Table1: Influence of genetic variations in CYP2D6 and/or CYP2C19 on doxepin metabolism and drug response.
| Phenotypes | CYP2D6 Diplotypes | Study Size | Country | Dose | Findings | Reference |
|---|---|---|---|---|---|---|
| EM (8), IM (8), PM (8) | *1/*1 (8), *1/*4 (7), *1/*5 (1), *4/*4 (6), *4/*5 (1), *3/*5 (1) | 24 | Germany | 75 mg (SD) | Mean E-doxepin clearance (95% CI) was 406 (390-445), 247 (241-271), and 127 (124-139) l/h in EMs, IMs and PMs of CYP2D6. The E,Z doxepin median oral clearance (l/h*kg) differed 4-fold between EM (6.2) and PM (1.4, p=<0.001). The PM had a more than 4-fold and 3-fold elevated AUC (0-48h) (micromol*h/l) for N-desmethyldoxepin (PM: 5.28 (2.62-21.66) vs EM: 1.28 (0.81-1.63) p=0.002) and doxepin active moiety (PM: 4.15 (2.49-8.87) vs EM: 1.43 (0.95-1.97) p<0.001). PM had a nearly 2-fold higher N-desmethyldoxepin plasma Cmax (nmol/l) (PM: 45 (29-87) vs EM: 26 (20-40) p=0.008) and a 3-fold prolonged elimination half-life of N-desmethyldoxepin (h) (PM: 79 (50-172) vs EM: 27 (16-45) p<0.001). The pharmacokinetic data for IM are between those of EM and PM. The bioavailability was 50 % greater in PM due to CYP2D6 activity toward E-doxepin. | 12360109 |
| UM (11), EM (11), PM (3) | *1x2/*1 (1), *2x2/*1 (2), *1x2/*35 (1), *2x2/*35 (1), *35x2/*1 (1), *2x2/*41 (1), *1x2/*41 (1), *1x2/*10 (1), *1x2/*9 (1), *41x2/*2 (1), *1/*35 (1), *1/*2 (2), *1/*1 (4), *35/*41 (1), *2/*41 (1), *1/*10 (1), *1/*9 (1), *4/*4 (2), *3/*3 (1) | 25 | Germany | 75 mg (SD) | The geometric mean (95% CI) of doxepin total oral clearances in the UM, EM and PM groups were 708 (458-1155), 251 (177-357) and 102 (77-137) l/h and the corresponding data for the doxepin maximum plasma concentrations were 26 (19-36), 35 (26-47), and 100 (66-150) nmol/l. The pharmacokinetics of N-desmethyldoxepin also depended on the CYP2D6 genotype with mean AUCs of 200 (114-349), 562 (439-721), and 1820 (1210-2737) in the UM, EM and PM group (p=0.003 for the EM versus UM, t-test). A trend (p=0.07, t-test) for lower AUC of the sum of doxepin and N-desmethyldoxepin in UM (575 (377-877)) vs EM (1000 (780-1282)) was found - UM had 0.5 of the AUC in EM. In a stereoselective analysis an effect of the UM genotype was found on E-doxepin PK parameters but no effect on the Z-doxepin PK. | 16007002 |
| PM (1) | *3/*4 (1) | 1 | Finland | N/A | Post mortem toxicology case of fatal doxepin poisoning. The blood concentration of doxepin was 2.4 mg/l, which is 16-80 times higher than therapeutic concentrations (0.03-0.15 mg/l). The concentration of desmethyldoxepin was high with 2.9 mg/l, which is not consistent with acute intoxication. | 17721180 |
| PM (1) | Not reported | 4 received doxepin | not reported | Study with 9 different antidepressants (TCA, SSRI, SNRI). Polymorphisms in CYP2D6, CYP2C19, and CYP2C9 were investigated with regards to an association with drug plasma concentration (sum of doxepin and desmethyldoxepin was measured). 136 patients in total, 4 were on doxepin, doxepin median plasma concentration was 0.2697 (0.1943-0.64) (ng/ml/mg). One patient was CYP2D6 PM. For the CYP2D6 PM patient deviation from median plasma concentration is -12%, HAMD changed from 29 at the first visit to 12 at the last visit, the CGI 1 drop by 2 from the first to the last visit and the CGI 2 at the last visit was 3, the patient experienced relevant side effects at the first visit. No information for the other 3 patients on doxepin. No further conclusion since study focused on all antidepressants. | 15168101 | |
| Phenotypes | CYP2C19 Diplotypes | Study Size | Country | Dose | Findings | Reference |
| EM (8), IM (7), PM (6) | *1/*1 (8), *1/*2 (7), *2/*2 (6) | 21 | Germany | 75 mg (SD) | The median oral clearance of doxepin (Z-doxepin) differed 2 fold between EM and PM. No effect on N-desmethyldoxepin concentration-courses in plasma was found. Desmethyldoxepin was detected in CYP2C19 PM. | 12360109 |
EM: extensive metabolizer; IM: intermediate metabolizer; PM: poor metabolizer; UM: ultrarapid metabolizer
Edit history (3)
- 2012-10-29 Create
- 2025-03-24 Update fixed typos
- 2025-07-17 Update fixed link