About this pathway
Introduction
Clomipramine is a chlorinated analogue of the tricyclic antidepressant (TCA) imipramine. It is used in the treatment of obsessive-compulsive and depression disorder. Its pharmacokinetics, pharmacodynamics, and pharmacogenetics are less well documented as compared to more frequently used TCAs amitriptyline or imipramine/desipramine.
Pharmacokinetics
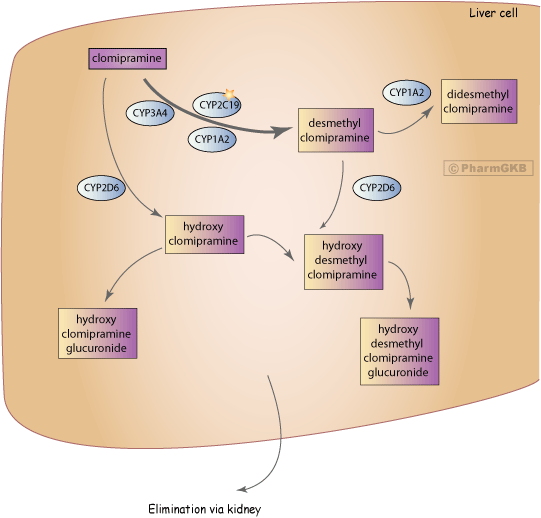
As with other tricyclics, clomipramine undergoes considerable biotransformation before excretion. A major route of its hepatic first pass metabolism is the demethylation into desmethyl clomipramine by several cytochrome P450 enzymes (CYP), including CYP2C19 (shown in in-vivo studies) [Articles:20531370, 11763000] and CYP3A4 and CYP1A2 (shown in in-vitro studies) [Articles:8667235, 10375803, 15168101]. Additionally, plasma concentrations of clomipramine were significantly lower in smokers than in nonsmokers indicating a role for smoking-induced CYP1A2 [Articles:7202824, 10353456]. Desmethyl clomipramine is an active metabolite. It is a stronger inhibitor of norepinephrine reuptake and weaker inhibitor of serotonin reuptake, compared to the parent drug clomipramine [Article:2044329]. Both the parent drug and the active metabolite undergo hydroxylation catalyzed by CYP2D6 to 8-hydroxy desmethyl clomipramine, 8-hydroxy clomipramine, 2-hydroxy clomipramine and 2-hydroxy desmethyl clomipramine (see Figure). The 2- and 8-hydroxylated metabolites are excreted predominantly renal in the form of glucuronide conjugates [Articles:7859811, 1451721]. Additionally desmethyl clomipramine is further demethylated to didesmethyl clomipramine [Article:7903373].
The elimination half-life is about 24h for clomipramine and 96h for desmethyl clomipramine. The time to reach steady-state concentration is in general around 3 weeks [Article:2044329].
As with other TCAs, clomipramine plasma concentrations show a wide range of inter-individual variation. Studies find a statistically significant difference in metabolic ratio or dose between patients suffering from drug side effects and patients with a good drug tolerance [Articles:15252821, 15168101, 10460069]. The potential influence of genetic variations in CYP2D6 and/or CYP2C19 is evaluated in several studies and the results are summarized below and in Table1.
Only two studies have investigated the effect of variations in both CYP2D6 and CYP2C19 on clomipramine metabolism. The investigation of CYP2C19 and CYP2D6 gene variation on the metabolism of amitriptyline, citalopram and clomipramine found no significant effect of CYP2C19*2 or *17 on the metabolic ratio for clomipramine but for amitriptyline and citalopram in a Caucasian population [Article:20531370]. The same study shows that increasing semi-quantitative gene dose values of CYP2D6 correlates with decreasing metabolic ratio for clomipramine to desmethyl clomipramine [Article:20531370]. Another study in Japanese patients shows that subjects homozygous for mutated alleles of CYP2C19 have higher clomipramine concentration and a higher value of clomipramine/desmethyl clomipramine ratio compared with those who were homozygous for wild-type alleles [Article:11763000]. Regarding the variation in the CYP2D6 gene, no significant difference in the ratio of desmethy clomipramine/hydroxy desmethyl clomipramin was observed between intermediate and extensive metabolizer phenotypess [Article:11763000]. Neither of the studies reported effects on response to clomipramine or side effects.
Few more studies report on the effect of CYP2D6 variation. CYP2D6 ultrarapid metabolizers were found to have low plasma concentrations of clomipramine and desmethyl clomipramine and no response to the clomipramine standard dose. Treatment response is reported after a dose increase to 300 mg/day clomipramine [Article:8093319] or addition of a second antidepressant [Article:9562213]. In case reports of CYP2D6 poor metabolizer patients higher clomipramine and desmethyl clomipramine steady state concentration compared to standard level were measured, which resulted in report of side effects [Articles:16871470, 2741190, 3582462]. In a study of Caucasian depressed patients, CYP2D6 intermediate metabolizers have a higher risk for side effects than extensive metabolizer [Article:15252821].
Co-administration of the neuroleptic levomepromazine, a potent inhibitor of CYP2D6, results in higher levels of desmethyl clomipramine and clomipramine compared to patients only taking clomipramine or in addition with benzodiazepine [Article:2880723]. The main effect of neuroleptics on tricyclic antidepressant metabolism seems to be the inhibition of their hydroxylation by CYP2D6, leading to a marked increase in their steady-state plasma concentrations.
Pharmacodynamics
The mechanism of action is still unknown but one effect is the increase in serotonin levels primarily through inhibition of serotonin reuptake. In animal studies clomipramine had marked affinity for 5-hydroxytryptamine (serotonin) receptor 2A (HTR2A), 2C (HRT2C), adrenoceptor alpha 1B (ADRA1), as well as modest affinity for dopamine receptor D2 (DRD2), D3 (DRD3), adrenoceptor alpha 2A (ADRA2), 5-hydroxytryptamine (serotonin) receptor 3A (HTR3) [Article:574454]. Clomipramine also displayed high affinity for both histamine receptor H1 (HRH1) and cholinergic receptor, muscarinic 1 (CHRM1) [Article:574454]. Clomipramine seems to influence the HPA axis via the central nervous system as measured by stimulation of cortisol secretion [Article:6093182].
Few studies have investigated the influence of variation in primarily pharmacodynamic genes on response to clomipramine in patients with depression or obsessive-compulsive disorder (Table2). Clomipramine-induced prolactin release was significantly greater in healthy subjects with the 44-base-pair insertion of the 5-HTTLPR (rs4795541) polymorphism in the promoter region of the solute carrier family 6 (neurotransmitter transporter, serotonin), member 4 (SLC6A4) gene. This suggests that subjects with the homozygous deletion genotype may have a poorer therapeutic response to clomipramine [Article:10867985]. No association of response to clomipramine and genetic variation in SLC6A4, solute carrier family 6 (neurotransmitter transporter, dopamine), member 3 (SLC6A3), solute carrier family 6 (neurotransmitter transporter, noradrenalin), member 2 (SLC6A2), 5-hydroxytryptamine (serotonin) receptor 1B (HTR1B), HTR2A, and catechol-O-methyltransferase (COMT) in patients with obsessive-compulsive disorder has been reported [Article:21625751]. A study investigating the association of antidepressant medication and suicide found that higher clomipramine and desmethyl clomipramine levels were significantly associated with higher treatment increasing suicidal ideation. A lower value for the desmethy clomipramine/clomipramine metabolite ratio was significantly associated with increasing suicidal ideation [Article:21449676]. Variants in the FK506 binding protein 5 (FKBP5) and ATP-binding cassette, sub-family B (MDR/TAP), member 1 (ABCB1) were the strongest genetic predictors for increased risk of suicidal ideation [Article:21449676].
Table 1: Influence of genetic variations in CYP2D6 and/or CYP2C19 on clomipramine metabolism and drug response.
| Phenotypes | CYP2D6 Diplotypes | Study Size | Ethnicity | Dose | Findings | Reference |
|---|---|---|---|---|---|---|
| UM (3); EM (85); IM (56); PM (7) | CYP2D6*3, *4, *5, *6, and multiplication genotyped but diplotypes not further specified in paper | 151 | Dutch | 25-300 mg/day | Compared to the EM group PMs, IMs, and UMs showed no significant difference in dose, steady state plasma concentration (Css) of clomipramine (C) and desmethyl clomipramine (DC). Also PMs showed no difference in dose adjusted Css C (both 1,2 g/l per mg/day) and a decrease in ratio of Css C/DC by 63% (1,6 to 0,6). IMs showed an increase in dose adjusted Css C by 50% (1,2 to 1,8 g/l per mg/day). UMs showed a decrease in dose adjusted Css of C by 25% (1,2 to 0,9 g/l per mg/day). | 20531370 |
| EM; IM | *1/*1 (8), *1/*2 (4), *2/*2 (1), *1/*10 (17), *2/*10 (9),*1/*5 (1), *2/*5 (2), *10/*10 (9) | 51 | Japanese | 10-250 mg/day | Compared to EM group with wild-type alleles (ratio steady state plasma concentration (Css) desmethyl clomipramine (DC)/hydroxy desmethyl clomipramine (HDC) = 1.94), the *10/*10 carrier had a ratio Css DC/HDC of 1.72 and the carrier of one mutant allele (*5 or *10) had a ratio Css DC/HDC of 1.77. | 11763000 |
| EM (20); IM (25) | 1/*2 (20); *1/*4 (25) | 45 | Caucasian | 100-150 mg/day for 3 week | The percentage of patients with side effects increased from 30% to 56% in the IM group compared to EM. The mean CYP2D6 activity was lower in the group with side effects. Dextrorphan/dextromethorphan ratios of 5.5 and 13.3 in the groups with and without side effects respectively. | 15252821 |
| EM (97); PM(12) | n/a | 109 | White | 25-200 mg/day | Serum levels of clomipramine + desmethyl clomipramine showed weak correlation with depression ratings. Blood pressure measurements and ratings of typical side-effects showed a statistically significant dose-effect and concentration-effect relationship. (Phenotyped with sparteine) | 10460069 |
| EM (15); PM (10) | n/a | 25 | 100 mg single dose | Compared to the EM group PMs had clearance decreased from 98.6 to 65.2 l/hr and t½ increased from 18.7 to 22.7 hour. (Phenotyped with sparteine) | 8181196 | |
| EM (35); PM (1) | n/a | 36 | Danish | 75 mg | The PM subject showed the following parameter changes compared to the EMs: steady state plasma concentration (Css) clomipramine (C)+desmethyl clomipramine (DC) increased from 710 to 2120 nM, Css C increased from 200 to 570 nM; ratio Css C/DC was unchanged, ratio of C/hydroxy clomipramine (HC) increased from 1.9 to 4.7, ratio of DC/hydroxy desmethyl clomipramine (HDC) increased from 1.6 to 7.1, the ratio (C+DC)/(HC+HDC) increased from 1.7 to 6.1. (Phenotyped with sparteine) | 1451721 |
| PM (1) | *4/*6 | 1 | not reported | 225-300 mg/day | A 47-year-old male patient experienced multiple adverse drug reactions during therapy with clomipramine (C) 225-300 mg/day and quetiapine 700 mg/day. Drug serum concentrations of C and quetiapine were significantly increased. Steady state plasma concentration (Css) of C + desmethyl clomipramine (DC) was 1228 ng/ml (therapeutic range 175-400 ng/ml). Genotyping showed a PM status for CYP2D6 (*4/*6), low CYP3A4/5 activity and normal CYP2C19 genotype (EM). After reduction of the C dose to 75mg/day and discontinuation of quetiapine, all adverse drug reactions subsided except for the increase in liver enzymes. Css C+DC was decreased to 374ng/ml. | 16871470 |
| PM (2) | not reported | 2 | not reported | 150 and 225 mg/day | Patient 1 received clomipramine (C) 150 mg/day for 3 weeks. No clinical improvement was observed but side effects were reported. The steady state plasma concentration (Css) of C + desmethyl clomipramine (DC) was 1215ng/ml, Css of C was 235ng/ml, and Css of DC was 980 ng/ml. Patient 2 received C 225 mg/day for 8 weeks. No clinical improvement was observed but severe side effects were reported. The Css for C+DC was 1120ng/ml, Css for C 160 ng/ml, and for DC 960 ng/ml. | 2741190 |
| PM (1) | not reported | 1 | not reported | 100 mg/day | Patient received clomipramine (C) 100 mg/day for 2 months and blood concentrations were analyzed at 2 time-points: steady state plasma concentration (Css) of C and desmethyl clomipramine (DC) were 598 ng/ml and 558 ng/ml. Compared to the reference values of this laboratory (125-350 ng/ml) this was an increase by 135-152%. Increased concentrations were mainly the result of increased DC concentration. The Css C is increased by 6-14% compared to the mean reference values (25-100 ng/ml). | 3582462 |
| UM (1) | not reported | 1 | not reported | 150-225 mg/day | A 62-year-old patient who did not respond to various antidepressants over a ten-year period. He had unusual low plasma concentrations of clomipramine (C) + desmethyl clomipramine (DC) during treatment with C 150-225 mg/day. C concentration increased fivefold after addition of 100 mg/day fluvoxamine and he showed rapid and consistent response to the treatment. The patient was found to have a duplication of the CYP2D6 gene. | 9562213 |
| UM (1) | not reported | 1 | not reported | 150-225 mg/day | A patient with agoraphobia was treated with 150 mg/day clomipramine (C) daily. Since there was no response, the dose was increased to 225 mg/day. Plasma concentrations were much lower than expected with 150 nM for C and desmethyl clomipramine (DC) concentration was below the level of quantitation (<100 nM). The patient was stabilized on 300 mg/day C. | 8093319 |
| Phenotypes | CYP2C19 Diplotypes | Study Size | Ehnicity | Dose | Findings | Reference |
| not reported | *1/*1 (70), *1/*17 (47), *17/*17 (4), *2/*2 (3), *1/*2 (20), *2/*17 (7) | 151 | Dutch | 25-300 mg/day | CYP2C19 status was not significantly associated with dose, steady state plasma concentration (Css) clomipramine (C), Css desmethyl clomipramine (DC). Metabolic ratio of C/DC was significantly increased (1,4 to 2,5) for CYP2C19 *2/*2 vs CYP2C19 *1/*1. Within the CYP2D6*1/*1 subgroup the differences in daily dose reached significance for subgroup CYP2C19*17/*17 vs CYP2C19*1/*1. | 20531370 |
| no mutation (18), one mutation (25), two mutations (8) | *1/*1 (18), *1/*2 (15), *1/ *3 (10), *2/*2 (5), *2/*3 (3) | 51 | Japanese | 10-250 mg/day | Compared to carrying no mutation patients with one mutation (*2 or *3) show significantly increased dose and weight adjusted steady state plasma concentration (Css) (from 57.4 ng/ml/kg to 81.2 ng/ml/kg) and the ratio of Css of clomipramine (C)/desmethy clomipramine(DC) is significantly increased (from 0.81 to 1.17). Patients homozygous for *2 or*2 and *3 show significantly increased dose and weight adjusted Css (from 57.4 ng/ml/kg to 100.8 ng/ml/kg) and the ratio of Css of C/DC is significantly increased (from 0.81 to 1.36). | 11763000 |
EM: extensive metabolizer; IM: intermediate metabolizer; PM: poor metabolizer; UM: ultrarapid metabolizer
Table 2: Influence of variation in primarily pharmacodynamic genes on drug response or side effects in patients with depression or obsessive-compulsive disorder treated with clomipramine.
| rs number | Gene | associated | allele | Dose | Study Size | Ethnicity or Country | Findings | Reference |
|---|---|---|---|---|---|---|---|---|
| rs1360780 | FKBP5 | yes | T | 50-300 mg/day | 74 | European ancestry | Carriers of the T allele, taking clomipramine or other antidepressants, are at a higher risk of treatment increasing suicidal ideation | 21449676 |
| rs2032582 | ABCB1 | yes | T | 50-300 mg/day | 74 | European ancestry | Carriers of the T allele, taking clomipramine or other antidepressants, are at a higher risk of treatment increasing suicidal ideation | 21449676 |
| rs130058 | HTR1B | yes | T | 50-300 mg/day | 74 | European ancestry | Carriers of the T allele, taking clomipramine or other antidepressants, are at a higher risk of treatment increasing suicidal ideation | 21449676 |
| rs4795541 | SLC6A4 | yes | ins | 0.1mg/kg | 14 | UK | Carriers of the 44 bp insertion have a greater clomipramine-induced prolactin release | 10867985 |
| rs4795541 | SLC6A4 | no | 235.5 (±40.8) mg/day | 41 | Brazil | no association with clomipramine response in obsessive-compulsive patients | 21625751 | |
| rs57098334 | SLC6A4 | no | 235.5 (±40.8) mg/day | 41 | Brazil | no association with clomipramine response in obsessive-compulsive patients | 21625751 | |
| rs6296 | HTR1B | no | 235.5 (±40.8) mg/day | 41 | Brazil | no association with clomipramine response in obsessive-compulsive patients | 21625751 | |
| rs6113 | HTR2A | no | 235.5 (±40.8) mg/day | 41 | Brazil | no association with clomipramine response in obsessive-compulsive patients | 21625751 | |
| rs6305 | HTR2A | no | 235.5 (±40.8) mg/day | 41 | Brazil | no association with clomipramine response in obsessive-compulsive patients | 21625751 | |
| rs4680 | COMT | no | 235.5 (±40.8) mg/day | 41 | Brazil | no association with clomipramine response in obsessive-compulsive patients | 21625751 | |
| rs5569 | SLC6A3 | no | 235.5 (±40.8) mg/day | 41 | Brazil | no association with clomipramine response in obsessive-compulsive patients | 21625751 |
Edit history (1)
- 2014-02-06 Create