About this pathway
BACKGROUND
Nevirapine (NVP) is a non-nucleoside reverse transcriptase inhibitor (NNRTI) used in combination with other antiretroviral (ARV) drugs for the treatment of human immunodeficiency virus (HIV) type 1 (HIV-1) infection. It is widely used in resource-limited settings [Articles:20696882, 22301417, 21969039]. Nevirapine inhibits reverse transcriptase enzyme, an essential viral enzyme that transcribes viral RNA into DNA, by binding to the enzyme, specifically to tyrosines at amino acid residues 181 and 188 which are located near the catalytic site [Articles:7533197, 8452345]. Nevirapine is not effective against HIV-2, as the pocket of the HIV-2 reverse transcriptase has a different structure, which confers intrinsic resistance to the NNRTI class.
Pharmacokinetics
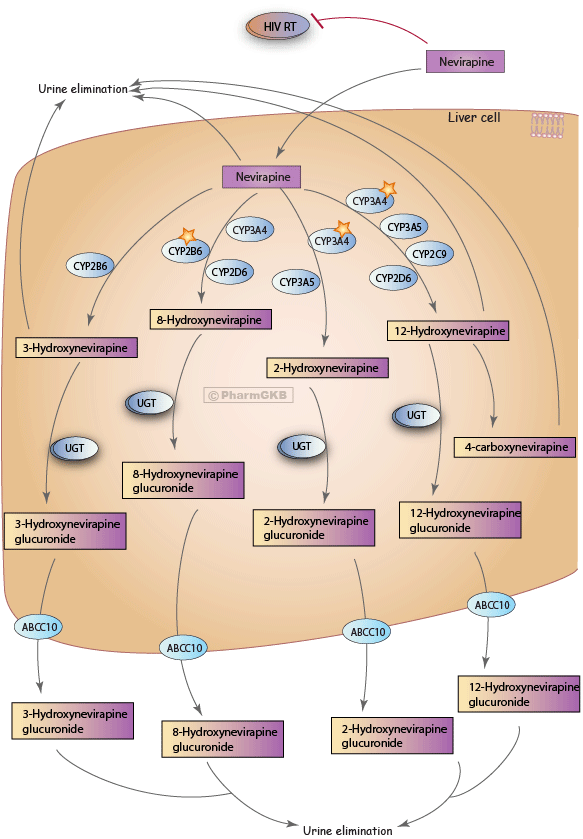
After oral administration, NVP is readily absorbed (>90%) and freely partitions to all tissues, including the brain, due to its low level of protein binding. Hepatic metabolism of NVP is mainly through induction of CYP enzymes 3A4 and 2B6, leading to formation of 2-, 3-, 8-, and 12-hydroxynevirapine followed by glucuronidation of these hydroxyl metabolites by UGT enzymes [Article:10421616] and urinary excretion. Other CYP enzymes, CYP3A5, CYP2C9 and CYP2D6 play a minor role [Articles:10570031, 19364830]. Auto-induction also results in a corresponding decrease in the terminal-phase half-life of NVP in plasma, from approximately 45 h (single dose) [Article:21920159] to approximately 25 - 30 h (multiple dosing with 200 - 400 mg/day). Induction is complete within 28 days and the resultant steady-state plasma nevirapine trough concentrations of 4.7 mg/ml (interquartile range: 3.6 - 6.4 mg/ml) are stable for at least one year of therapy [Article:18729332].
The metabolites 2- and 3-hydroxyNVP are primarily formed by CYP3A4 and CYP2B6, respectively [Article:21441248] and CYP3A4 plays a role in the biotransformation of both 8- and 12-hydroxyNVP [Articles:10570031, 10421616]. The 2-, 3-, and 8-hydroxylation can lead to formation of para-quinone imine intermediates after further oxidation. The metabolite 12-hydroxynevirapine has the potential to be sulfated followed by loss of sulfate to form a reactive quinone methide [Article:18729332]. Further oxidation of 12-hydroxynevirapine by ALDH results in formation of 4-carboxynevirapine [Articles:10421616, 18729332, 19364830]. Drug transporters expressed in key target tissues may have a role in drug intake and efflux, but little is known about the transporters that influence the disposition of nevirapine. However, the multidrug resistance protein 7, encoded by the adenosine triphosphate-binding cassette gene ABCC10, has been implicated in the efflux process of the metabolites [Article:22082652].
Pharmacogenetics
Nevirapine has been associated with serious and sometimes life threatening rash and/or hepatotoxicity during the first 6 to 18 weeks of therapy [Articles:22301417, 18729332, 19364830, 16912957, 21969039, 20017669]. The clinical impact of the CYP2B6 polymorphism, 516G>T, rs3745274, on NVP pharmacokinetics has been described in various settings [Articles:21441248, 22354160, 20017669, 22111602, 21393201, 21860339]. The use of single-dose NVP to prevent perinatal vertical transmission has been shown to have pro-longed exposures in women with the CYP2B6 516 T allele, which greatly increases the risk of developing resistance mutations to NVP [Article:19812066]. Individuals with the CYP2B6 *6/*6 or *6/*18 haplotype have been shown to have a significant increase in NVP plasma concentrations [Article:22354160]. The 983T>C SNP (rs28399499) which results in an amino acid change in the CYP2B6 protein (Ile328Thr), has also been shown to impact upon NVP pharmacokinetics [Articles:18281305, 21441248].
Data from other studies show that nevirapine induces its metabolism by CYP3A4/5 and CYP2B6 through the activation of the nuclear receptor, constitutive androstane receptor (CAR; NR1I3) [Article:17041008]. The nuclear receptor pregnane X receptor (PXR; NR1I2) regulates basal expression of CYP3A4/5 [Article:17925385]. Polymorphisms in the genes coding for these nuclear receptors have been shown to influence the expression of the CYPs and therefore influence nevirapine exposure [Articles:16101575, 17041008, 17925385]. The NR1I2 6-bp indel, which is in linkage disequilibrium with NR1I2 44477T>C, is associated with lower nevirapine exposures, which may indicate increased basal expression of CYP3A4 [Article:22111602]. The possible role for P-glycoprotein, encoded by the ATP-binding cassette transporter gene, ABCB1 in NVP pharmacodynamics still remains unclear. However, the ABCB1 c.3435C>T SNP has been found to be involved, and the 3435T allele has been significantly associated with decreased risk of hepatotoxicity with NVP-containing regimens [Articles:20017669, 16912957]. One of the genome-wide association analysis and replication studies of candidate SNPs identified significant associations of nevirapine-induced rash with 2 SNPs (rs1265112 and rs746647) within the CCHCR1 gene [Article:21810746]. Multiple HLA loci have been implicated in NVP cutaneous adverse events (HLA-B*35 and HLA-Cw*04) and hepatic adverse events (HLA-DRB1*01 and HLA-DQB1*05) [Article:21505298].
Edit history (1)
- 2012-03-21 Create