About this pathway
Background
The thiopurine drugs are purine antimetabolites widely used in the treatment of acute lymphoblastic leukemia, autoimmune disorders (e.g., Crohn’s disease and Rheumatoid Arthritis) and of organ transplant recipients (reviewed in [Articles:16550163, 26067482]). They were one of the first drugs studied for their pharmacogenomic (PGx) response [Article:7191632][Article:8644731], one of the earliest to have PGx added to the drug label [Article:17108808] and to have guidelines from the Clinical Pharmacogenomics Implementation Committee (CPIC) [Article:21270794]. Side effects for thiopurine drugs range from mild rash, flu-like symptoms to severe life-threatening myelosuppression and hepatotoxicity [Article:26876431]. Incidence of side effects in IBD populations ranges from 0-39% and is increased in Asian populations [Article:18557712]. The thiopurine drugs were first developed as drugs in the 1950s by Hitchings and Elion [Article:14907641]. The papers that make up the bones of this pathway, ie. which metabolites are formed, date back to these times, are often not available online in full text. These can be found referenced in the components tab or Pathvisio pathway data files rather than as references in this text. Since this text focuses on the PGx of thiopurines as it relates to the pathway, it tends to reference newer papers that discuss the candidate genes involved in the processes, and which are generally available online.
Pharmacokinetics
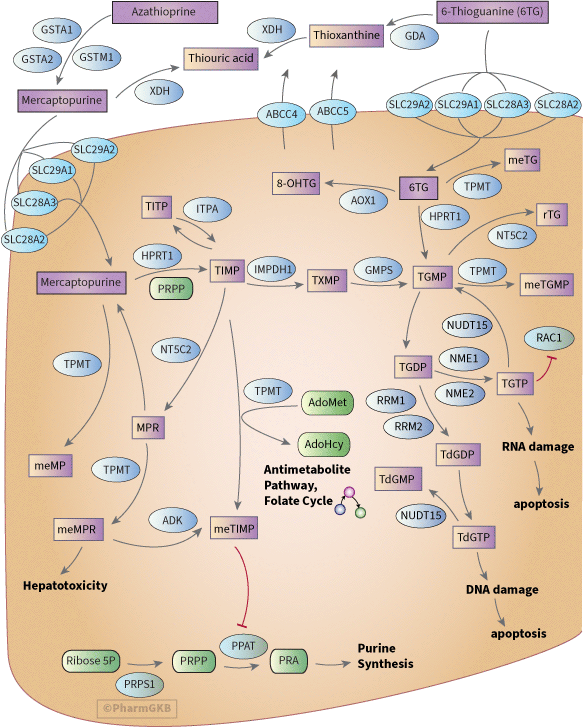
As inactive prodrugs, 6-mercaptopurine (6-MP), 6-thioguanine (6-TG) and azathioprine (AZA) require intracellular activation, catalyzed by multiple enzymes, to exert cytotoxicity. The first step in AZA activation is the release of 6-MP. While the drug label mentions non-enzymatic conversion, published work in vitro suggests this accounts for less than 1% of all biotransformation [Article:16717136]. GSTM1, GSTA1 and GSTA2 are all capable of metabolizing AZA at physiologically relevant levels [Article:16717136]. While GSTA2 had the highest activity against AZA, it is expressed at lower levels than GSTA1 and GSTM1, and so considered that their contributions to the biotransformation of azathioprine will be quantitatively similar in individuals of normal expression [Article:16717136]. GSTM1 is a highly polymorphic gene and there are individuals with no expression (null variant) and those with multiple gene copies (for more details on this variant see VIP and for AZA specific PGx see below). GSTA3, GSTA4, GSTK1 and GSTM2 all had low activity (an order of magnitude lower than GSTA1), GSTP1 and GSTT1 had no activity [Article:16717136]. Candidates for the transport of thiopurines into the cell include SLC28A2 (CNT2), SLC28A3 (CNT3), SLC29A1 (ENT1) and SLC29A2 (ENT2) [Articles:17996297, 16530731]. Cell lines resistant to 6-MP and 6-TG have down-regulated influx transporters [Articles:16530731, 17996297, 21723252]. Resistance can also be conferred by overactive efflux of thiopurines and their metabolites from the cell by ABCC4 and ABCC5 [Articles:12435799, 10840050, 17996297]. Variants in ABCC4 can affect sensitivity to thiopurines and influence their toxicity (discussed further in PGx section below)[Articles:18593894, 20393862]. After uptake, 6-MP is converted into thioinosine monophosphate (TIMP) by HPRT1, with 5-phospho-D-ribose-1-pyrophosphate (PRPP) as the phosphoribosyl donor. In a similar way, 6-TG can be converted into thioguanosine monophosphate (TGMP). TGMP can also be formed from TIMP in two steps: first, thioxanthosine monophosphate (TXMP) is formed by IMPDH; second, TGMP is formed by GMPS [Article:18662289]. Subsequently, TGMP can be converted into active metabolites thioguanine nucleotide diphosphate (TGDP) and triphosphate (TGTP) and incorporated into RNA (see PD section below), this is carried out by nucleoside diphosphate kinases NME1 and NME2 [Article:20216118]. TGDP can be converted to TdGDP and incorporated into DNA [Article:1157053]. The formation of TdGDP is probably carried out by ribonucleotide reductase (coded for by genes RRM1, RRM2, and RRM2B)(described but not referenced or shown in [Article:22662200]). These enzymes normally catalyze GDP to dGDP and although direct evidence for their action on specific thioguanines is lacking, azathioprine and RRM1 are documented to interact suggesting that binding of TGDP to RRM1 would not be blocked by the thiol moiety [Article:22662200]. TIMP can be shunted away from formation of TGTP to MPR by NT5C2 or methylTGMP by TPMT or 8-OHTG by AOX1 [Article:10525111]. In a study of pediatric leukemia patients receiving continuous infused TG, 8-OHTG was the major circulating metabolite [Article:10525111]. On the 6MP side of the pathway there are also branches that lead away from the formation of damaged RNA and DNA; oxidation of 6MP by XDH to form thiouric acid (extracellular) [Article:24415675], and methylation by TPMT (intracellular)[Article:24415675]. TG can also form thiouric acid in a two step process action by guanine deaminase, GDA, forming thioxanthine followed by oxidation by XDH [Article:10525111].
Pharmacodynamics
Cytotoxic effects of thiopurine drugs are achieved through four routes:
- incorporation of thio-deoxyguanosine triphosphate (TdGTP) into DNA
- incorporation of TGTP into RNA
- inhibition of de novo purine synthesis by methylmercaptopurine nucleotides (mainly meTIMP) [Article:23811272]
- inhibition of Rac1 by TGTP (this inhibition induces apoptosis in activated T cells) [Article:16365460].
Incorporation of TdGTP into DNA inhibits the function of several enzymes involved in DNA replication and repair. It also induces DNA damage such as single strand-breaks, DNA-protein cross-links and chromatid exchanges [Articles:6204746, 7682415, 10606189]. In the same way incorporation of thioguanine nucleotides (TGNs) into RNA leads to damage. This damage to RNA and DNA ultimately results in cytotoxicity and apoptosis.
Relative amounts through each of the pharmacodynamics sub-pathways impacts the efficacy and toxicity of thiopurines. For use in inflammatory disease TGNs are considered the pharmacologically active metabolites and meMP [Articles:28130685, 22261533],meMPR and 6MMPR (methyl mercaptopurine ribonucleotides which includes meTIMP and meTGMP) [Articles:27943397, 25853923] are associated with hepatotoxicity.
Pharmacogenomics
TPMT
The most extensively studied gene in the context of thiopurine PGx is TPMT. Thiopurine PGx is discussed in detail in the TPMT VIP and clinical annotations and variant annotations are available for the key variants and haplotypes [Article:20154640]. The CPIC guidelines give clinical PGx information as well as background data on TPMT allele frequencies and distribution in different racial and ethnic groups [Articles:21270794, 23422873]. Although homozygous inactivating variants of TPMT are highly predictive of thiopurine related toxicity (100% positive predictive value) [Article:21270794], TPMT variants are relatively rare: approximately 5% in White populations, 3% in Asian populations and 6% in Black populations [Article:23422873], and homozygotes are in the range of 1 in 178 to 1 in 3,736 patients [Articles:23422873, 21270794].
Other genes and variants that contribute to variable toxicity:
NUDT15
First identified by GWAS of IBD patients [Article:25108385] and also in children with acute lymphoblastic leukemia (PMID 25624441), NUDT15 variant rs116855232 T was associated with thiopurine-related hematopoietic toxicity. This candidate gene has been confirmed in several other studies to be associated with thiopurines tolerance and/or thiopurine-related toxicity in both IBD and leukemia patients [Articles:26878724, 26405151, 26033531, 26503813, 26735160, 26590936, 26076924]. The frequency of the T allele ranges from 1-10% in HapMap populations shown at dbSNP.
NUDT15 converts the active metabolites TdGTP and TGTP to the inactive TdGMP and TGMP respectively, preventing the incorporation of TdGTP into DNA and TGTP into RNA [Article:25624441].
ITPA
Several studies have examined the role of ITPA variants in thiopurine metabolism, dose, efficacy and toxicity; however, results have been somewhat contradictory reflecting the complex nature of this pathway and how different branches may have more relevance with the different drugs or underlying conditions or population. Most studies examined the 94C>A variant (rs1127354) which has a frequency of 3-10% in HapMap populations with lower frequency in African populations and higher frequencies in Asian populations see tables at dbSNP. Studies of ITPA in pediatric leukemia patients have shown association of ITPA 94A with hematological or myelotoxicity (leukopenia, neutropenia, anemia) [Article:26237184][Article:18685564] although one study in Asian patients did not see association [Article:26405151]. ITPA 94A was associated with increased methylmercaptopurine, levels of which are associated with increased likelihood of hepatotoxicity [Article:21395650]. This was most significant in those without TPMT variants. The impact of the variant on hepatotoxicity directly was not stated but the study size was small and may not have had power to detect this (n=65) [Article:21395650]. A 2007 meta-analysis of 6 studies of Caucasian adult IBD patients concluded that there was insufficient evidence for ITPA 94C>A to predict toxicity. Studies that did show positive association included a study of IBD patients receiving azathioprine (n=262) in the Netherlands where the A allele was associated with increased likelihood of leukopenia [Article:16431304], and a study from the UK of adult IBD patients receiving azathioprine (n=207) where ITPA 94A was associated with a flu-like set of symptoms but not any other ADR including neutropenia [Article:18616518]. A study of Japanese IBD patients suggests that 94A may have decreased risk for leukopenia 94A was associated with lower 6-TGNs but the authors did not examine the role of this variant alone on leukopenia and when in combination with ABCC4 rs3765534 T (which has higher risk for leukopenia) the result was neutral [Article:20393862]. Intronic variant of ITPA rs7270101 SNP in ITPA has been reported to alter splicing and is associated with decreased ITPA expression and enzyme activity reduced ITPA expression in tumor cells results in thiopurine resistance. [Article:24624911]. decreased survival associated with ITPA polymorphisms reported in Asian ALL patients.
ABCC4
Several variants for ABCC4 were shown in a GWAS to be influential to thiopurine metabolism and cellular phenotypes [Article:24624911]. The variant rs3765534 C>T is a non-synonymous variant resulting in a protein change of Glu757Lys. Cells with the rs3765534 TT variant genotype (as reported on the plus chromosomal strand for this minus strand gene) had greater sensitivity to 6MP toxicity. Cells with the TT variant were less able to exclude 6-MP metabolites compared to the reference allele due to lower cell surface expression [Article:18593894]. This was confirmed in a study of Japanese IBD patients, where rs3765534 TT and CT genotypes were associated with decreased white blood cell counts, increased 6-TGNs and increased likelihood of Leukopenia when treated with azathioprine or mercaptopurine compared to CC genotype [Article:20393862]. A study of Japanese pediatric ALL patients found those who were homozygous for the minor allele of any of ABCC4 variants rs3765534, rs2274407 or rs11568658 required a lower daily dose [Article:25403995] Results for the coding change p.Lys304Asn rs2274407C>A are contradictory. In a study of white Canadian pediatric ALL patients co-treated with 6MP and methotrexate, the AC genotype was associated with increased thrombocytopenia and decreased EFS compared to CC genotype [Article:19515727], definitely. A study of pediatric ALL patients from Egypt, also treated with 6MP and MTX reported the opposite relationship where CC was associated with increased myelotoxicity compared to AA and AC (neutropenia and leukopenia)[Article:26237184]. Further functional studies of this variant may clarify its role.
Other genes
Various other genes and variants have been shown in single studies to influence thiopurine phenotypes including AOX1 [Article:19500084], PACSIN2 [Article:22846425], HLA isotypes [Article:25217962], microRNAs [Article:23358152], ATP6AP2, GNG2, FRMD4B, NME1, UTP18 and KCNMA1 [Article:24624911] and others. These are described in variant annotations under the PGx tab.
Note This figure has been updated in 2017 to included newer candidate genes not depicted in the published figure from 2010.
Reactions & interactions (91)
-
Biochemical Reaction
mercaptopurine → thiouric acid
-
Biochemical Reaction
thioguanine → 8-hydroxythioguanine
-
Biochemical Reaction
mercaptopurine riboside → mercaptopurine
-
Biochemical Reaction
thioguanine → thioxanthine
-
Biochemical Reaction
thioguanosine monophosphate → methyl-thioguanosine monophosphate
-
Biochemical Reaction
thioguanosine monophosphate → thioguanosine diphosphate
-
Biochemical Reaction
s-adenosylmethionine + thioinosine monophosphate → methyl-thioinosine monophosphate + s-adenosylhomocysteine
-
Biochemical Reaction
thioinosine monophosphate → thioxanthine monophosphate
-
Biochemical Reaction
6-methylmercaptopurine riboside → methyl-thioinosine monophosphate
-
Biochemical Reaction
thioguanosine triphosphate → thioguanosine monophosphate
-
Biochemical Reaction
thioguanine → methylthioguanine
-
Biochemical Reaction
thioinosine monophosphate → thioinosine triphosphate
-
Biochemical Reaction
thioxanthine monophosphate → thioguanosine monophosphate
-
Biochemical Reaction
mercaptopurine → methylmercaptopurine
-
Biochemical Reaction
thioguanosine monophosphate → ribosylthioguanine
-
Biochemical Reaction
deoxy-thioguanosine diphosphate → deoxy-thioguanosine triphosphate
-
Biochemical Reaction
thioguanosine diphosphate → thioguanosine triphosphate
-
Biochemical Reaction
thioxanthine → thiouric acid
-
Biochemical Reaction
azathioprine → mercaptopurine
-
Biochemical Reaction
thioinosine monophosphate → mercaptopurine riboside
-
Biochemical Reaction
thioguanine → thioguanosine monophosphate
-
Biochemical Reaction
prpp → phosphoribosylamine
-
Biochemical Reaction
ribose phosphate → prpp
-
Biochemical Reaction
thioguanosine diphosphate → deoxy-thioguanosine diphosphate
-
Biochemical Reaction
mercaptopurine → thioinosine monophosphate
-
Biochemical Reaction
deoxy-thioguanosine triphosphate → deoxy-thioguanosine monophosphate
-
Biochemical Reaction
mercaptopurine riboside → 6-methylmercaptopurine riboside
-
Catalysis
XDH → Biochemical Reaction
-
Catalysis
AOX1 → Biochemical Reaction
-
Catalysis
GDA → Biochemical Reaction
-
Catalysis
TPMT → Biochemical Reaction
-
Catalysis
TPMT → Biochemical Reaction
-
Catalysis
IMPDH1 → Biochemical Reaction
-
Catalysis
ADK → Biochemical Reaction
-
Catalysis
NUDT15 → Biochemical Reaction
-
Catalysis
TPMT → Biochemical Reaction
-
Catalysis
ABCC4 → Transport
-
Catalysis
ABCC5 → Transport
-
Catalysis
ITPA → Biochemical Reaction
-
Catalysis
GMPS → Biochemical Reaction
-
Catalysis
ABCC4 → Transport
-
Catalysis
ABCC5 → Transport
-
Catalysis
TPMT → Biochemical Reaction
-
Catalysis
NT5C2 → Biochemical Reaction
-
Catalysis
SLC29A2 → Transport
-
Catalysis
SLC28A2 → Transport
-
Catalysis
SLC28A3 → Transport
-
Catalysis
SLC29A1 → Transport
-
Catalysis
NME2 → Biochemical Reaction
-
Catalysis
NME1 → Biochemical Reaction
- Showing first 50 of 91 reactions — full data preserved in database.
Edit history (7)
- 2004-12-02 Create
- 2008-10-15 Update
- 2017-03-17 Update Major Update including substantial addition of text and addition of gpml
- 2019-07-09 Update Updated to new illustrator format.
- 2025-04-10 Update fixed typo
- 2026-01-30 Update Updated image file to reverse arrow from meTIMP to go towards meTIMP, added arrow from 6TG to meTG with TPMT.
- 2026-02-02 Update Updated gpml to include methylthioguanine and arrow with TPMT and PMID:7603453