About this pathway
Background
Isoniazid (isonicotinic acid hydrazide, INH; PubChem ID 3767) [Article:18486045] is a first-line anti-mycobacterial agent used to treat active or latent tuberculosis (TB) infections generated by Mycobacterium tuberculosis [Articles:12588714, 16371463, 22467723]. INH has been in clinical use for over 60 years [Article:18486045] and standard regimens for active TB infections include two months treatment with INH, rifampicin, pyrazinamide and ethambutol or streptomycin, followed by an additional four months of INH and rifampicin treatment [Articles:10573254, 12588714, 16371463]. Management of latent TB infections typically involves administration of INH alone (for 6 or 9 months) or in combination with rifapentine (for 3 months) to individuals at high risk of developing active TB [Articles:16503745, 25201941]. Although effective, current therapeutic regimens are very lengthy and difficult to implement [Article:18486036], and TB remains a major global health problem with more than 9 million new cases and 1.5 million deaths reported in 2013 ISBN:9789241564809.
INH formulations are available as tablets (50, 100, or 300 mg) or solution (50 mg/5 ml) for oral administration, or as injection solution (100 mg/ml) for intramuscular use. Two combination formulations have additionally been approved for anti-TB therapy, Rifamate® (capsules with 150 mg INH and 300 mg rifampin) and Rifater® (tablets with 50 mg INH, 120 mg rifampin and 300 mg pyrazinamide) (Drugs@FDA). All drug labels begin with a boxed warning regarding hepatotoxicity associated with INH therapy; peripheral neuropathy is another common adverse reaction that can be avoided by co-administration of pyridoxine supplements to susceptible individuals (e.g. malnourished, pregnant/breastfeeding, etc.) [Articles:10573254, 12588714, 16371463]. Treatment-induced hepatotoxicity and other serious adverse reactions cause discontinuation in up to 10% of patients treated with standard regimens of first-line anti-TB drugs, including INH [Articles:8902462, 16503745, 24783247]. Patients who develop INH-induced hepatotoxicity present with symptoms such as abdominal pain, jaundice, nausea and vomiting, whereas features of drug hypersensitivity (e.g. fever, rash, arthralgia, eosinophilia) are rare [Articles:17021358, 16371463, 24783247]. Although extensively studied, the underlying mechanisms for INH-induced hepatotoxicity remain unclear [Article:21412230]. This is partly due to the complexity of these mechanisms, but also to the difficulty in distinguishing between drug-specific and patient-related factors that may determine susceptibility to INH toxicity [Article:25755470]. This manuscript outlines the basic aspects of INH absorption, distribution, metabolism and excretion (ADME) in humans, with special emphasis on the influence of genetic polymorphisms in genes encoding xenobiotic-metabolizing enzymes that modulate INH pharmacokinetics and, consequently, their association with INH-induced hepatotoxicity.
ADME/Pharmacokinetics
Few studies have been conducted investigating the in situ intestinal permeability of INH alone, though studies have been performed showing that INH has low permeability in the stomach and high permeability in the three segments of the small intestine (duodenum, jejunum, ileum) of rats [Articles:12921157, 15832504]. While the apparent permeability of the intestines and intestinal absorption rate constant of INH appears to decrease upon simultaneous perfusion with pyridoxine, no significant effects were concomitantly observed on INH pharmacokinetics [Article:23090666]. It is of note that the bioavailability of INH was not significantly affected in tuberculosis patients who had undergone surgical procedures involving resection of the stomach or parts of the intestinal tract [Articles:686569, 760100]. Absorption may be reduced by concomitant administration of sugar or following food intake. This is likely due to the conversion of INH to a hydrazone species, making it less available for absorption [Articles:5161562, 17117431, 20550762]. INH seems to be widely distributed to all fluids and tissues, according to the apparent value of distribution volume (0.6 L/kg on average), with the largest accumulation in the liver; the pharmacological model for INH seems to follow first-order kinetics (ISBN:9780911910001).
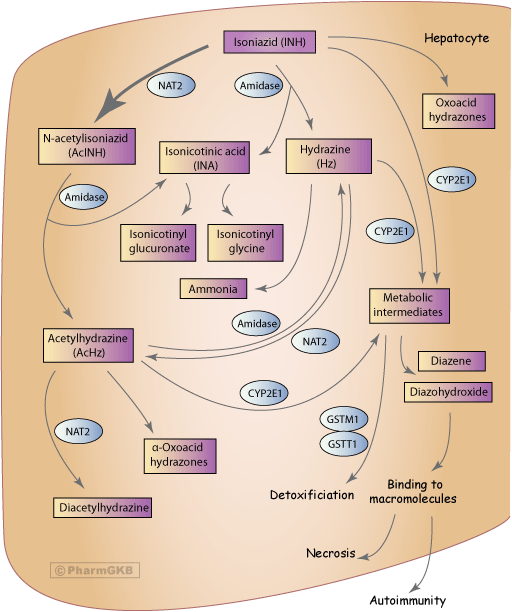
In the liver and intestines, INH is predominantly metabolized (50-90%) via N-acetylation of its hydrazine functionality by arylamine N-acetyltransferase 2 (NAT2; E.C. 2.3.1.5) to N-acetylisoniazid (AcINH) (Figure 1) [Articles:10746928, 18220565, 18544910, 17995946, 21412230, 22037847]. INH can also be hydrolyzed to hydrazine (Hz) by amidase with concomitant formation of isonicotinic acid (INA); it can also be metabolized into oxoacid hydrazone species [Articles:10215642, 18220565, 18544910, 17995946, 21412230, 22037847]. In turn, AcINH may be enzymatically hydrolyzed by amidase to form acetylhydrazine (AcHz) and INA [Articles:5075259, 950592, 10215642, 18220565, 17995946, 21412230, 22037847]. Additionally, AcHz can be deacetylated to Hz via hydrolysis by amidase or be further acetylated by NAT2 to diacetylhydrazine [Articles:10215642, 18220565, 17995946, 21412230, 21913872, 22037847]. Hz can be broken down to ammonia or acetylated to AcHz by NAT2 [Articles:18220565, 17995946, 22037847]. None of the metabolites have known antitubercular properties, apart from the hepatotoxic AcHz [Article:17117431].
INH, AcHz, and Hz are likely oxidized, in part, by cytochrome P450 2E1 (CYP2E1) into potentially hepatotoxic intermediates, however explicit evidence of this has not yet been found [Articles:21753138, 21913872, 23142471]. These intermediates can then be dehydrated into compounds that covalently bind with macromolecules in hepatocytes causing necrosis and, possibly, autoimmunity [Articles:1149365, 18220565, 21412230]. The glutathione S-transferase (GST) enzyme family can conjugate these potentially harmful metabolites with glutathione, effectively removing these toxic metabolites [Articles:11595069, 18544910, 21753138]. Similar to CYP2E1, there have not been any studies explicitly detailing the metabolism of INH accomplished by the GST enzymes [Article:11595069].
Urinary excretion is the primary elimination route (approximately 80%) of most INH metabolites (AcINH, AcHz, diacetylhydrazine) (ISBN:0962652350); INA may be excreted as a free acid metabolite or a conjugated species with glycine (isonicotinyl glycine) [Articles:18220565, 17995946, 22037847]. Less than 10% of the oral INH dose is excreted in the feces [Article:6391781].
INH and toxicity
Anti-tuberculosis treatment drug-induced liver injury (ATT-DILI) is an adverse reaction that may lead to poor compliance or interruption of treatment, and thus has implications for the control of TB infections [Articles:17021358, 24637014]. INH treatment is associated with increased activity of liver enzymes in 20% of patients and also with severe hepatotoxicity in 1-2% of patients [Articles:5361410, 5080707, 18295292, 24593909]. INH thus constitutes the leading cause of hepatotoxicity in many countries [Articles:5361410, 5080707, 18295292, 24593909]. A better understanding of the risk factors and mechanisms behind INH-induced hepatotoxicity may help in the prevention and mitigation of this complex drug reaction [Article:24593909]. Reported possible risk factors include advanced age, female sex/pregnancy, low body weight/malnutrition, alcoholism, pre-existing abnormal liver function/liver transplantation, co-administration with other hepatotoxic agents, chronic hepatitis B and C infection, AIDS, and genetic factors [Articles:17021358, 24593909]. No consistent associations between race and INH-induced hepatotoxicity are evident [Article:17021358]. Despite these postulated associations, the precise mechanism underlying INH-induced hepatotoxicity remains unclear; numerous different mechanisms are likely to be involved and influenced by multiple factors [Articles:17021358, 25755470, 24593909].
INH-induced hepatotoxicity has traditionally been attributed to the cytotoxic effects of INH metabolites, particularly AcHz and Hz [Articles:17995946, 21412230]. However, several features of this hepatotoxicity, such as a delay in liver injury after drug onset or the activation of macrophages by INH, are indicative of an immune response (see recent review by Metushi and colleagues for a thorough account of possible immune-related components of INH DILI) [Article:21412230]. A recent study also reported detection of covalent INH adducts with CYP2E1, CYP3A4 and CYP2C9 in the serum of INH-treated patients developing ATT-DILI, pointing to immunological response as the underlying mechanism of hepatotoxicity [Article:23775837].
As previously discussed, INH, AcHz, and Hz can be oxidized, potentially by CYP2E1, to hydroxyl-hydrazine intermediates that are then dehydrated to more damaging metabolites. These metabolites have the capacity to covalently bind macromolecules, causing liver injury [Articles:1149365, 18220565, 21412230, 25755470]. Hz and ammonia may also contribute to toxicity [Articles:18544910, 17995946, 21412230]. AcINH is less toxic than INH, but is not a potential therapeutic alternative due to its 100-fold less anti-mycobacterial activity and its ability to be hydrolyzed to hepatotoxic AcHz [Articles:18220565, 18544910, 17995946, 21412230, 22037847].
Mitochondrial abnormalities have been linked to the toxicity of an array of drugs [Article:18705745]. With respect to INH-induced hepatotoxicity, mitochondrial dysfunction appears to be caused by Hz, support for which comes from the observation that rat liver cells develop megamitochondria upon exposure to this particular metabolite prior to apoptosis. This finding is consistent with adaptive responses to oxidant stress and/or reduced oxygen consumption rates [Article:9895232]. Mechanistically, the finding that Hz inhibits the succinate dehydrogenase enzyme in a dose-dependent manner suggests that complex II and/or the tricarboxylic acid cycle may also be affected, but the nature of this effect is unclear [Article:23911619]. The various postulated mechanisms underlying the toxicological hazard posed by INH on liver cells have been extensively discussed recently [Article:24783247] and include oxidative stress and disruption of energy homeostasis attributable to mitochondrial damage.
It is also worth noting that INH is rarely administered alone and some of the toxic effects seen in patients treated with INH may be due to, or exacerbated by, drug-drug interactions [Articles:16503745, 17021358, 17545706, 20649602, 20564379, 23475203, 24783247, 25886055, 25988394].
Pharmacogenetics
As ATT-DILI remains unpredictable, even when environmental factors and drug regimen are considered, polymorphisms within genes involved in the INH pharmacokinetic pathway have been investigated in order to identify possible biomarkers for hepatotoxicity risk. These associations and the possible reasons behind a lack of consensus between studies are discussed below and summarized in Table 1.
NAT2
Studies unraveling the genetic basis of N-acetylation first appeared around 1990; an exhaustive review of INH acetylation pharmacogenetics in the NAT2 pre-genotyping era was published by Weber and Hein in 1985 [Article:2860675] and the subject has subsequently been reviewed by many authors, more recently by McDonagh and colleagues [Article:24892773]. When examining plasma concentrations of INH over time after an oral dose, a bimodal pattern was originally observed; higher plasma levels and reduced clearance of the drug were seen in slow acetylators compared to rapid acetylators. More refined phenotypic analysis further demonstrated a trimodal population distribution pattern; subjects can be divided into rapid, intermediate or slow acetylators [Article:2860675]. Following the development of genotyping techniques for the NAT2 gene, prediction of the acetylator phenotype has become possible through genetic testing. There are many different alleles described for the NAT2 gene (NAT Gene Nomenclature website) and an individual’s genotype can be predictive of rapid, slow or intermediate acetylator phenotype, depending on the presence of two "rapid" alleles, two "slow" alleles or one of each, respectively [Article:19018723]. The reference NAT2*4 allele is the most common NAT2 allele conferring the rapid acetylator phenotype and is associated with increased metabolism and clearance of INH [Articles:7773298, 21494681, 24892773]. Conversely, the polymorphic NAT2 alleles of the main allelic groups *5, *6, *7 and *14 encode for slow acetylator enzyme variants that may compromise the drug-metabolizing ability of individuals [Article:24892773].
An investigation of NAT2 genotype as a pharmacogenetic biomarker for personalization of INH therapeutic dosage demonstrated a linear relationship between clearance of the drug and the number (0 in slow, 1 in intermediate or 2 in rapid acetylators) of NAT2*4 alleles; this specific parameter accounted for 88% of the INH clearance variability observed in the Caucasian population studied [Article:15855489]. Similar conclusions were drawn by another study with Japanese TB patients treated with INH and rifampicin. Genotyped NAT2 slow acetylators (no *4 allele) exhibited significantly decreased acetylation of INH and Hz, resulting in increased serum concentrations of INH compared to intermediate (one *4 allele) or rapid (two *4 alleles) acetylators [Article:18544910]. Rapid acetylators display higher levels of AcINH and AcHz in serum and clear AcHz more quickly when compared to slow acetylators, whereas slow acetylators have higher exposure to AcHz and excrete more unchanged INH in urine [Articles:17021358, 18544910].
Apart from INH acetylation, NAT2 also catalyzes the acetylation of AcHz to non-toxic diacetylhydrazine [Article:2860675], and thus slow acetylator status causes accumulation of both Hz and AcHz to potentially hepatotoxic levels [Articles:7161842, 25755470]. Consequently, the NAT2 slow acetylator phenotype and genotype have been associated with an increased risk of INH-induced hepatotoxicity in the majority of published pharmacogenetic studies (Table 1); the patient cohorts genotyped are of various geographic origins, mainly from South America [Articles:18421452, 22012226, 22788240, 23190413, 23394127], East Asia [Articles:10751073, 11915035, 16246623, 17950035, 19891553, 20392357, 21753138, 22506592, 23407048, 24465778], South Asia [Articles:21261721, 23875638, 25017831, 24637014], Iran [Article:21047300], Turkey [Article:18330759] and Tunisia [Article:21856096]. The labels of all INH-containing drug formulations currently approved by the FDA inform that slow acetylators may have increased blood levels of the compound, which results in an increased risk of hepatotoxicity and peripheral neuropathy (Drugs@FDA). The NAT2 gene is included in the pharmacogenomic biomarkers list of the FDA in relation with INH, but no specific actions are recommended on the basis of this information.
Contradictory results regarding the acetylator status and risk of INH hepatotoxicity have also been reported in the literature. An early study [Article:1149365] attributed INH hepatotoxicity to the NAT2 rapid acetylator phenotype, presumably associated with increased plasma levels of AcHz. However, a series of ensuing pharmacological studies (reviewed by Weber and Hein [Article:2860675]) showed the opposite or no association between the acetylator phenotype and INH hepatotoxicity. A small number of recent studies have also reported no association between the acetylator genotype and INH-induced hepatotoxicity [Articles:16677176, 16770646, 19761367, 22283902, 22947533] (Table 1).
A recent clinical trial reported a significantly lower relative risk of unfavorable events in patients treated with an INH dose based on NAT2 genotype, compared to those treated with the standard dose, supporting a clinically-relevant association between NAT2 variants and INH pharmacokinetics [Article:23150149]. Importantly, in the genotype-based treatment group, efficacy of treatment in NAT2 slow acetylators was not reduced despite the lower doses administered. Also, incidence of INH-induced liver injury was not increased in rapid acetylators when INH was given in higher doses [Article:23150149]. More independent studies are required to verify these results.
With regard to individual NAT2 single nucleotide polymorphisms (SNPs), rs1799930 (NM_000015.2:c.590G>A, signature SNP for the NAT2*6 allelic group) has been associated with decreased acetylation of INH and clearance of the drug, which correlated with an enhanced risk of drug-induced hepatitis [Articles:18421452, 19891553, 25017831]. The NAT2*6 signature polymorphism has been reported to confer an ultra-slow acetylator phenotype [Articles:24221535, 25836746], and this could explain the higher risk of INH-induced hepatotoxicity in slow acetylators carrying this particular SNP. A slow acetylator haplotype composed of rs4646244 (NM_00015.2:c.-1144T>A) allele A, rs4646267 (NM_000015.2:c.-949A>G) allele A, rs1799930 allele A, and rs1799931 (NM_000015.2:c.857G>A, signature SNP for the NAT2*7 allelic group) allele G, has been associated with an increased risk of hepatotoxicity. Patients with this haplotype had significantly decreased acetylation and clearance of INH, as compared to the other haplotypes examined, and this is likely attributed to the presence of the ultra-slow NAT2*6 signature SNP [Article:19891553]. Another study has correlated genotype AA of rs1495741 (NC_000008.10:g.18272881G>A, a tag SNP located about 14 kb downstream of NAT2) with increased risk of INH hepatotoxicity [Article:23407048]. This association is indirect, as the A allele of rs1495741 is likely to be in linkage disequilibrium with a slow NAT2 variant [Article:20739907].
CYP2E1
CYP2E1 is involved in the oxidation of INH, AcHz, and Hz, resulting in likely hepatotoxic intermediates that undergo further dehydration to potentially harmful products [Articles:17950035, 18220565, 18544910, 21412230, 21753138, 21913872, 23142471]. Polymorphisms of the CYP2E1 gene have been examined in association with risk of INH-mediated ATT-DILI, mainly by investigators in South [Articles:16677176, 21261721, 23875638, 25017831, 24637014] and East [Articles:12668988, 17950035, 18544910, 19891553, 20392357, 20819434, 21753138, 22506592, 22335459, 24465778] Asia and South America [Articles:22012226, 22788240, 23190413, 23394127]. Although some studies have reported higher risk of ATT-DILI in INH-treated patients who bear high-activity alleles of CYP2E1, particularly *1A and *6 [Articles:12668988, 16677176, 16770646, 20819434, 21261721], other studies have found no association [Articles:17950035, 19891553, 19761367, 20392357, 20860460, 21753138, 22012226, 22506592, 22788240, 22335459, 23190413, 23875638, 25017831, 23394127, 24465778] and, therefore, a direct role for CYP2E1 in INH-induced hepatotoxicity remains widely controversial (Table 1). Evidence suggests that CYP2E1 polymorphisms may be associated with increased severity of INH related ATT-DILI, rather than enhanced susceptibility to it [Article:20392357]. Studies also report increased risk of ATT-DILI in INH-treated patients who combine high-activity CYP2E1 and slow NAT2 genotypes [Articles:12668988, 21261721, 22506592, 23394127, 24607341].
Since the generation of many INH metabolites does not depend exclusively on CYPs, attention has somewhat shifted away from CYP2E1 as a major predictor of hepatotoxicity [Articles:23142471, 24783247]. Nonetheless, the observation that CYP2E1 is expressed in mitochondria and is one of the CYP forms that generates relatively high levels of reactive oxygen species may point to a role for CYP2E1 in increasing the extent of oxidative stress [Articles:9114822, 21929725]. Moreover, anti-INH and anti-CYP2E1 antibodies have been found in the serum of patients with INH-induced liver failure; INH-CYP2E1 covalent adducts were also detected, as well as antibodies against them [Article:23775837]. Such auto-antibodies are considered markers of CYP2E1-directed autoimmunity, which may lead to liver injury [Article:25462068]. INH has been demonstrated to induce CYP2E1 enzyme activity [Article:8339754] and experiments with animal models support CYP2E1-mediated hepatotoxicity when INH is administered [Article:15132840].
GSTM1 and GSTT1
The GSTs are involved in the detoxification of numerous drugs and oxidative stress products; due to this role, polymorphisms of the GSTM1 and GSTT1 genes have also been investigated in risk of ATT-DILI [Article:20415545]. GSTs are known to be involved in the metabolism of anti-TB drugs via conjugation of potentially harmful metabolites; however, the specifics about this interaction are unknown [Articles:11595069, 21753138]. Deficiencies in GST activity due to homozygous null mutations in GSTM1 and GSTT1 may have the potential to modulate susceptibility to INH-induced hepatotoxicity [Article:25755470]. Indeed, several published studies have reported an association between GSTM1 homozygous null genotype and increased risk of ATT-DILI [Articles:11595069, 17400324, 18544910, 24114827], although the majority of studies report no association found [Articles:18397238, 20853551, 20036620, 20819434, 21753138, 22012226, 22788240, 22335459, 24465778] (Table 1). A similar pattern is seen for the GSTT1 homozygous null genotype, with one study from Spain describing an association with increased risk of ATT-DILI [Article:18397238], but the majority of studies (in Asia or Brazil) reporting no association [Articles:11595069, 17400324, 20853551, 20036620, 21753138, 22012226, 22788240, 22335459, 24114827, 24465778] (Table 1). Studies have also shown an additive effect of combined GSTM1 and GSTT1 null genotypes on risk of INH hepatotoxicity [Articles:24114827, 24637014], as well as of combined NAT2, CYP2E1, GSTM1 and/or GSTT1 polymorphic genotypes [Article:22788240]. There does not seem to be a consistent pattern of factors that indicate why these contradictory results have been observed.
Other genes
It is likely that multiple genetic factors and gene-gene interactions are involved in INH-induced hepatotoxicity risk, as is the case for other hepatotoxic drugs [Article:23360680]. Indeed, significant associations with risk have been reported for genotypes of other genes [Articles:17400324, 22341855] (Table 1), which further complicates the assessment of possible risk factors. INH liver injury was associated with certain major histocompatibility complex (MHC) class II alleles, including human leukocyte antigen (HLA) haplotypes, which supports the role of the immune system in INH toxicity [Article:21412230]. The absence of the HLA-DQA1*0102 allele and the presence of the HLA-DQB1*0201 allele were reported to be independently associated with increased risk of ATT-DILI in 331 TB patients [Article:12359646]; however, the Bonferroni correction introduced to compare the distribution of both alleles in ATT-DILI and non-ATT-DILI patients could only confirm the negative association of DQA1*0102 with ATT-DILI, but was not clearly explained. Generally, only some cases of ATT-DILI associated with INH are suggested to be immune-mediated and HLA-associated, which may explain the discrepancy observed in some studies [Article:21412230]. Overall, a direct association of ATT-DILI with HLA alleles may be difficult or not possible to establish at this stage [Article:12359643].
One study in Japanese patients found associations between INH-induced hepatotoxicity and particular polymorphisms in the genes involved in one of the antioxidant pathways. Among these positive correlations, one polymorphism in NOS2A, which encodes inducible nitric oxide synthase, causes an increase in nitric oxide production. Polymorphisms in BACH1 (encoding basic leucine zipper transcription factor 1) and MAFK (encoding v-maf avian musculoaponeurotic fibrosarcoma oncogene homologue K) result in suppression of the nuclear factor erythroid 2-like 2 (Nrf2) pathway [Article:22341855] (Table 1). However, it remains mechanistically unclear how these mutations may contribute to ATT-DILI.
Meta-analyses of NAT2, CYP2E1, GSTM1 and GSTT1 genotypes
Several meta-analyses have been published to examine the association between ATT-DILI and genetic variants of drug metabolizing enzymes. A large meta-analysis of 38 studies found NAT2 slow acetylator genotype to be significantly associated with risk of ATT-DILI [Article:23082213]. A meta-analysis of 4 studies found an association between increased risk of ATT-DILI and NAT2 slow acetylator status (defined as non-carrier of the *4 allele, as opposed to rapid acetylator status defined as heterozygous or homozygous for *4) in TB patients of Asian ethnicity (OR=2.52, CI=1.49-4.26, p-value not provided) [Article:18713495]. However, in another larger meta-analysis with some overlapping studies, a significant association between ATT-DILI and NAT2 slow acetylator status was observed in both Asian and non-Asian patients [Article:22409928]. The same meta-analysis, which also analyzed different treatment combinations, found a significantly increased risk of ATT-DILI with NAT2 slow acetylator status compared to the rapid status in patients treated with INH, rifampicin, pyrazinamide and ethambutol (9 studies, OR=4.09, 95% CI=2.78-6.03, p<0.001), or INH and rifampicin (3 studies, OR=34.30, 95% CI=10.41-113.00, p<0.001), but not with INH only (2 studies, OR=2.36, 95% CI=0.52-10.73, p<0.266) [Article:22409928].
One meta-analysis showed that the CYP2E1*1A/*1A high-activity genotype is significantly associated with risk of ATT-DILI, but only in East Asian patients [Article:23082213]. CYP2E1*1A/*1A genotype was significantly associated with increased risk of ATT-DILI compared to all other genotypes in a meta-analysis of 4 studies (OR=2.22, 95% CI=1.06-4.66, p=0.03) [Article:18713495]. Finally, the CYP2E1*1A/*1A genotype was determined to be a risk factor for ATT-DILI, particularly when combined with the slow acetylator NAT2 genotype (OR=3.10, 95% CI=1.83-5.26. p<0.0001) [Article:24607341].
While two meta-analyses have shown significant associations of the GSTM1 null genotype with risk of ATT-DILI, neither meta-analysis found such an association for the GSTT1 null genotype [Articles:18713495, 23082213]. A recent large-scale meta-analysis of GST variants, which included 13 and 12 case-control studies for the GSTM1 and GSTT1 null genotypes, respectively (approximately 900 cases and 1900 controls for each gene), found evidence that the null genotype of GSTM1, but not GSTT1, was associated with marginally increased susceptibility to ATT-DILI [Article:23377313], which was consistent with the previous meta-analyses [Articles:18713495, 23082213].
Conclusion
The current consensus among the literature is that one mechanism is unlikely to explain INH-induced hepatotoxicity and that numerous pathways are probably involved. Different drug-specific mechanisms have been suggested, but most supporting data have been generated from cellular and animal models and thus do not account for the multitude of factors that may contribute to susceptibility to INH-induced hepatotoxicity in clinical settings. Variants of enzymes involved in the INH metabolic pathway have been associated with ATT-DILI, particularly the slow acetylator variant of NAT2. However, upon comparing studies in Table 1, there does not seem to be an obvious underlying factor that explains why some studies found an association and others did not; it is likely that many factors, such as inconsistent genotyping and phenotyping methods, study design, anti-TB drug regimen and the overall condition of patients, may contribute to risk of INH-induced hepatotoxicity. Future investigations that utilize DNA sequencing may lead to further identification of variants contributing to ATT-DILI. Large-scale, robust analyses of these underlying genetic and environmental risk factors in clinical settings will help uncover the full picture of these important and complex adverse reactions.
Reactions & interactions (28)
-
Biochemical Reaction
hydrazine → acethydrazide
-
Biochemical Reaction
acethydrazide → diacetylhydrazine
-
Biochemical Reaction
isoniazid metabolic intermediates → isoniazid diazene metabolite
-
Biochemical Reaction
isonicotinic acid → isonicotinyl glucuronate
-
Biochemical Reaction
isoniazid → acetylisoniazid
-
Biochemical Reaction
isoniazid → isonicotinic acid
-
Biochemical Reaction
hydrazine → isoniazid metabolic intermediates
-
Biochemical Reaction
acetylisoniazid → acethydrazide
-
Biochemical Reaction
isonicotinic acid → isonicotinyl glycine
-
Biochemical Reaction
isoniazid → hydrazine
-
Biochemical Reaction
acethydrazide → isoniazid hydrazones
-
Biochemical Reaction
acethydrazide → isoniazid metabolic intermediates
-
Biochemical Reaction
acetylisoniazid → isonicotinic acid
-
Biochemical Reaction
isoniazid metabolic intermediates → isoniazid diazohydroxide metabolite
-
Biochemical Reaction
isoniazid → isoniazid metabolic intermediates
-
Biochemical Reaction
acethydrazide → hydrazine
-
Biochemical Reaction
hydrazine → ammonia
-
Biochemical Reaction
isoniazid → isoniazid hydrazones
-
Catalysis
NAT2 → Biochemical Reaction
-
Catalysis
NAT2 → Biochemical Reaction
-
Catalysis
NAT2 → Biochemical Reaction
-
Catalysis
CYP2E1 → Biochemical Reaction
-
Catalysis
CYP2E1 → Biochemical Reaction
-
Catalysis
CYP2E1 → Biochemical Reaction
-
Leads To
isoniazid diazohydroxide metabolite → Toxic liver disease
-
Leads To
GSTM1 → Detoxification
-
Leads To
GSTT1 → Detoxification
-
Leads To
isoniazid metabolic intermediates → Detoxification
Edit history (1)
- 2025-02-28 Update Fixed broken gpml. There are still a few unlinked components.