About this pathway
Atomoxetine (ATX) is a norepinephrine reuptake inhibitor used for the treatment of attention-deficit hyperactivity disorder (ADHD). ATX affects the norepinephrine pathway by inhibiting the norepinephrine transporter (SLC6A2) in the presynapse, however the complete mechanism of action is not entirely understood [Articles:8233054, 25637266]. It has a relatively low affinity profile for other neuronal transporters and neurotransmitter receptors compared to tricyclics [Article:6123593]. It seems that the blood-brain-barrier transport of ATX is predominantly passive [Article:18936112] and ATX is unlikely a substrate of ABCB1 [Article:17963743].
Pharmacokinetics
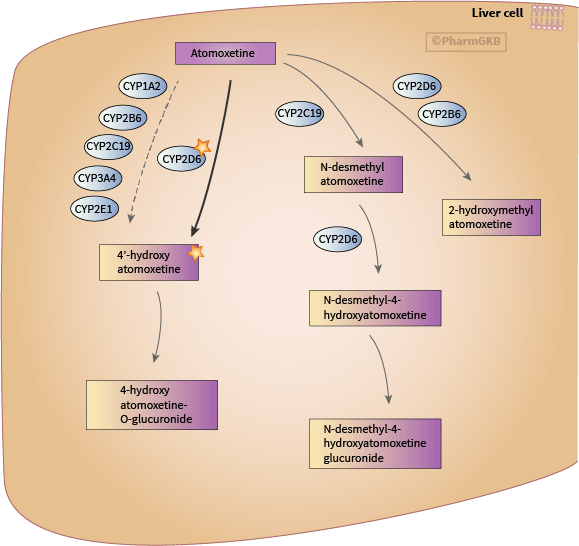
Pharmacokinetics studies in healthy individuals suggest that an enzyme with polymorphic alterations is involved in the clearance of ATX since 2 out of the 11 participants showed a prolonged half-life time and subsequent accumulation of ATX upon multiple dosing [Article:4008676]. 4-hydroxyatomoxetine (4-OH ATX) is the major and also pharmacological active metabolite of ATX, which is rapidly glucuronidated to the inactive 4-hydroxyatomoxetine glucuronide (4-OH ATX glucuronide) [Article:12485958]. Studies using human liver microsomes demonstrate that 4-OH ATX formation correlates with CYP2D6 activity [Articles:11854152, 27052878]. Multiple CYPs (CYP1A2, CYP2B6, CYP2C19, CYP3A4, CYP2E1) showed to be capable to form 4-OH ATX in microsomes deficient of CYP2D6. However, the efficiency is reduced and the amount of metabolite is less than mediate by CYP2D6 [Article:11854152]. In contrast, screening several heterologously expressed CYP 450 enzymes only identifies CYP2J2 as minor enzyme (100-fold lower than CYP2D6) for the 4-OH ATX formation [Article:27052878]. However, in the same study, the identification of inhibitors of the 4-OH ATX formation in pooled human liver microsomes shows only quinidine (CYP2D6) contributed in a dose-depended manner. In addition, ketoconazole (CYP3A) inhibited the 4-OH ATX formation in liver microsomes of a subject with no CYP2D6 activity [Article:27052878]. A less prominent route of the ATX elimination is the transformation to the inactive N-desmethylatomoxetine (N-desmethyl ATX; noratomoxetine) by CYP2C19 and further formation of N-desmethyl-4-hydroxyatomoxetine presumably through CYP2D6 [Articles:12485958, 11854152, 26660002]. N-desmethyl ATX was also generated by CYP1A1, CYP2B6, CYP2D6, CYP2J2, CYP3A4 and to the greatest content by CYP2C18 in an experiment using heterologously expressed cytochrome P450 [Article:27052878]. Additionally, 2-hydroxymethylatomoxetine (2-CH2-OH-ATX) and 2-hydroxymethylatomoxetine derived metabolites are detected in small amounts [Articles:12485958, 26660002]. For the transformation of ATX to 2-CH2-OH-ATX, CYP2D6 and CYP2B6 might be involved [Article:27052878].
Pharmacogenomics
Radioactive labeled ATX was well absorbed from the GI tract with no inter-individual differences. In subjects with full CYP2D6 metabolism the majority of the radioactive dose is excreted within 24 h (ATX t1/2=5h), while in subjects with CYP2D6 deficiency the excretion time is increased to 72h (ATX t1/2=20h) [Article:12485958]. Four-OH ATX glucuronide accounted for about 84% of the total radioactivity in urine samples and 67% in plasma samples of subjects with functional CYP2D6 after 5 days twice 20mg ATX and one dose of 14C-ATX on day 6 [Article:12485958]. The amount in urine is reduced in the CYP2D6 poor metabolizer (PM) subjects (31%) but 4-OH ATX glucuronide is still the primary ATX-derived metabolite in urine 120-264h post administration. In plasma samples of the PM subjects, concentrations of ATX and N-desmethyl ATX were the most abundant metabolites [Article:12485958]. Since CYP2D6 is indicated in the clearance of N-desmethyl ATX the higher amount of this metabolite in CYP2D6 PMs is thought to be the result of accumulation due to slower clearance rather than enhanced production. The study finds an increase of metabolites from secondary (minor) transformation routes in CYP2D6 PM subjects (22% of the ATX dose) compared to CYP2D6 normal metabolizers (NM; former extensive metabolizer) (3% of the ATX dose) [Article:12485958]. A single ATX dose study in 23 children confirms 4-OH ATX as the predominate metabolite, primarily glucuroniated, independent from the CYP2D6 genotype. The N-demethylation route only contributes minimally in the ATX metabolism but N-desmethyl ATX is found in higher percentage in PM compared to NM subjects and an increase in metabolites from secondary routes in PM is also in agreement with the study in adults [Article:26660002].
The majority of ATX pharmacogenetic studies published today investigate the effect of CYP2D6 variation. Table 1 summarizes studies, which compare efficacy and side effects in child and adolescent patients grouped by carriers of two no function CYP2D6 alleles (PM) vs remaining subjects. The no function alleles *3, *4, *5, *6, *7, *8 were determined. Homozygous and compound heterozygous carriers of these alleles were classified as PM while heterozygous and non-carriers were grouped as NM. PMs achieve a 2- to 5 times higher average peak plasma concentration of ATX than CYP2D6 NMs [Articles:12562062, 17242628]. At an ATX dose of at least 1.2mg/kg/day no differences in treatment discontinuation is found comparing 1290 NMs vs. 67 PMs or 1239 NMs vs 87 PMs [Articles:12562062, 17698328]. However, a different analysis of several combined studies points towards a higher rate of study continuation in PMs (2563 NM vs 171 PM, p=0.032, Fisher exact test). It was argued that this was driven by increased efficacy shown through better improvement based on the attention deficit–hyperactivity disorder rating scale (ADHDRS) [Article:17242628], while another study could not demonstrate a difference in response between the two groups [Article:17698328]. CYP2D6 PMs develop a slightly higher increase in pulse rate and more weight loss than NMs [Articles:12562062, 17242628, 17698328]. No difference regarding the QT interval is observed between CYP2D6 NM and PM child and adolescent patients [Articles:17242628, 17698328].
Besides the larger studies described above additional pharmacogenetics studies about the effect of CYP2D6 variation on atomoxetine pharmacokinetic parameter and outcome/ADR are summarized in Table 2. Using only CYP2D6 PM (no specific variants reported), healthy adult subjects dosed with placebo, 40 and 120mg/day ATX (maximum approved dose on a weight adjusted basis) show a significant increase in heart rate corrected QT interval (QTc) with increasing plasma concentrations [Article:22803597]. However, the authors conclude that ATX is not associated with clinically significant change in QTc [Article:22803597]. Higher incidences of abrasion (p=0.013) and tremor (p<0.001) are reported in children with the PM phenotype compared to NM [Article:17242628]. In adults treated with ATX 80-100 mg/day, a higher frequency of dry mouth, erectile dysfunction in men, hyperhidrosis, insomnia and urinary retention is reported comparing PM vs non-PM [Article:25919121]. While in the study in children only no function alleles were interrogated, the later study in adults further looked at other metabolizer phenotypes and cannot establish differences for treatment-emergent adverse events between NM/ultrarapid metabolizers (UM) and intermediate metabolizers (IM) (see Table 2) [Article:25919121]. However, the IM group encompasses a wide range of functionality binning patients with one normal and one reduced or no function allele, two reduced function alleles, and one reduced and one no function allele.
A recent single dose study with 0.5 mg/kg ATX in children grouped the subjects in NMs with either one or two normal function or two decreased function alleles, IM (carriers of one decreased and on no function allele) and PM (two no function allele) [Article:26660002]. The plasma concentrations of ATX and 4-OH ATX and the oral clearance of ATX are significantly different between PM and NM subjects but the IM values did not significantly differ from PM for some but not all parameters assessed. The dose-corrected ATX systematic exposure varied 29.6 fold across the cohort of 23 children and is CYP2D6 genotype dependent with 4.4±2.7 µM*h in NMs with 2 or more functional alleles to 5.8±1.7 µM*h, 16.3±2.9 µM*h and 50.2±7.3 µM*h in NMs with two decreased function alleles or one normal and one no function allele, IMs and PMs, respectively (p<0.0001) [Article:26660002]. Studies in Asian populations show that the pharmacokinetic parameters of ATX such as Cmax, AUC and clearance differ between *1/*1, *1/*10, and *10/*10 carriers (Table 2) [Articles:17610534, 21543662, 26254792] but the clinically significance of this variance is not investigated. In two small studies no differences in tolerance of ATX is found [Articles:17610534, 21543662].
Besides variation in CYP2D6, co-medication with CYP2D6 inhibitors might affect ATX pharmacokinetics. Paroxetine increased C(ss,max), AUC0-12, and t1/2 of atomoxetine by approximately 3.5-, 6.5-, and 2.5-fold, respectively in a study in 22 healthy individuals treated with 20mg/day ATX to steady state and additional 20mg/day paroxetine. After co-administration with paroxetine, increases in N-desmethyl ATX and decreases in 4-OH ATX concentrations were observed [Article:12412820]. Similarly, Kim et al. reports an effect of paroxetine co-administration on ATX pharmacokinetic parameters [Article:27673638]. In addition, a case study reports symptom improvement through elevation of ATX concentrations due to paroxetine co-administration [Article:18215333].
The product labels of several agencies contain information about CYP2D6 and atomoxetine, and are summarized on the ATX drug label page.
Although most pharmacogenetic studies exist for CYP2D6 variations in association with efficacy and risk of side effects of ATX treatment, a few studies about CYP2C19 and SLC6A2 variants have been published. A study in 40 healthy Korean subjects showed a difference in pharmacokinetic parameters of ATX after a single dose of 40 mg. ATX plasma concentrations (Cmax and AUC) were higher, the clearance (CL/F) was lower and the half-life time longer in CYP2C19 PM (carriers of *2/ *2, *2/ *3, *3/ *3) compared to IM (*1/ *2, *1/ *3) and NM (*1/ *1) [Article:24346747]. N-desmethyl ATX plasma concentrations (Cmax and AUC) were lower in comparison. All patients were CYP2D6 *1/*10 [Article:24346747].
Studying the target of ATX, Ramoz et al. used two different cohorts (N=160 and N=105) of children with ADHD [Article:19387424]. The treatment of the patients in the first cohort is initiated at a dose of 0.5 mg/kg/day and could be titrated to a maximum dose of 1.8 mg/kg per day of atomoxetine for the duration of up to 10 weeks of acute, open-label treatment. The second, smaller cohort used an acute, randomized, double- blind treatment of 0.8–1.8 mg/kg per day of atomoxetine for 6 weeks. From the initially studied 108 SNV across SLC6A2 14 are nominal significant in the combined cohort of 265 patients. However, none of these 14 variants are showing significance regarding an association with response after 6 weeks of treatment in all analyses such as cohort1, cohort2, combined cohort, and Caucasian subjects only. The strongest association with response measured through a combined scale of attention-deficit/hyperactivity disorder rating scale (ADHDRS) and clinical global impressions-severity of illness scale (CGI-S) scores was detected for the T allele of rs3785152 (p<0.01, odds ratio (OR) 2.2 for the combined cohort; p<0.01 OR 3.1 for cohort 1; p<0.01 OR 2.7 for Caucasians only; p=0.15 OR 2.1 for cohort 2) [Article:19387424]. Yang et al. finds an association of rs3785143 T allele with being a non-responder in a cohort of 111 Chinese children with ADHD treated with a dose titrated to 1.2-1.4 mg/kg per day and maintained for 4 weeks (p=0.0416, OR 2.66, after multiple test correction) [Article:23266789]. Attention-deficit/hyperactivity disorder rating scale version 4 (ADHDRS-IV) score is used in this study as primary efficacy measure and a 25% reduction in score defines responders. The result for SLC6A2 rs3785143 could not be replicated and shows no difference between responders and non-responders [Article:23266789].
Conclusion
ATX is extensively metabolized by the highly variable CYP2D6. This leads to considerably variability in drug exposure at recommended doses.
Table 1
Efficacy and side effects in child and adolescent patients (mixed ethnicities) grouped by carriers of two no function CYP2D6 alleles (poor metabolizer; PM; e.g.*4/*5) vs normal metabolizer (NM; e.g. *1/*4, *1/*1). The cohorts were genotype for *3, *4, *5, *6, *7, *8, decreased function alleles were not included.
| Published studies/meta-analyses | Original studies | Size | Dose (administered) | Dose (final) | Response (ADHDRS-IV-Parent:Inv score) | Discontinuation | ADR general | Weight and pulse | QT interval |
|---|---|---|---|---|---|---|---|---|---|
| 12562062 | Allen AJ et al 2001 (no PMID) | 1290NM; 67 PM | At least 1.2 mg/kg/day | No difference | No difference | higher increase in pulse rate and weight loss in PM than NM (no statistics) | |||
| 17242628 | 11694667; 12411225; 12523874 | 559 NM; 30 PM | Weight-adjusted basis to a maximum total daily dose of 1.8 mg/kg | PM: mean final dose 1.28 (0.36) mg/kg/day NM: 1.37 (0.33) mg/kg/day (p = 0.12) | Greater improvements for PM compared with NM by mean final ADHDRS total scores (p=0.002) and higher rate of responder (p=0.033) | ||||
| 17242628 | Not reported | 2563 NM; 171 PM | Received a dose >1.2 mg/kg/day | PM: mean final dose was 1.51 (0.30) mg/kg/day NM: 1.55 (0.29) mg/kg/day | Treatment discontinuations (p=0.032) attributed to a lack of efficacy (p=0.004) were significantly lower for PM as compared with NM, no difference in discontinuations due to ADR | No difference except higher incidences of abrasion (p=0.013) and tremor (p<0.001) are reported in PM vs EM | Greater increase in pulse (p<0.001) and diastolic blood pressure (p<0.012) and less weight gain (p=0.088), for PM compared with NM | No differences | |
| 17698328 | Allen AJ et al 2001 (no PMID); Wernicke et al 2002 (no PMID) | 1239 NM; 87 PM | Initiated at 0.5 mg/kg/day and increased up to 1.8 mg/kg/day during trial with the goal to reached CGI-ADHD-S score below 3 | Mean final doses (at endpoint) were NM: 1.50 mg/kg/d (SD = 0.36) and PM: 1.35 mg/kg/d (SD = 0.43) p=0.004 | Non-significant higher total score reduction in PMs (p=0.07) and responder rate did not differ (p=0.56) | No difference in discontinuations (p=0.33); trend of higher discontinuation rates due to any adverse event among PM (NM: 30 of 1239, or 2.4%; PM: 5 of 87, or 5.8%, p=0.08) | Weight differences with weight loss in PM (p<0.001), and pulse increased more in PM than in NM (p<0.005) | No differences |
ADHDRS-IV-Parent:Inv: Attention-Deficit/Hyperactivity Disorder Rating Scale-IV-Parent Version: Investigator-Administered and –Scored; CGI-S: Clinical Global Impressions-Severity of Illness scale; CGI-ADHD-S: Clinical Global Impressions-ADHD-Severity; Responder: Response defined as a =25% decrease from baseline in ADHDRS-IV-Parent:Inv total score; NM: normal (former extensive) metabolizer; PM: poor metabolizer
Table 2
Influence of genetic variations in CYP2D6 on atomoxetine metabolism and drug response.
| Reference | CYP2D6 Phenotype | CYP2D6 Diplotype | Study Size | Country/Ethnicity | Dose | Major Findings |
|---|---|---|---|---|---|---|
| 11694667 | 280 NM, 17PM | NA (PM alleles genotyped) | 297 children and adolescents with ADHD | USA | placebo; 0.5; 1.2; 1.8 mg/kg/day | Efficacy was measured using ADHD RS scale score. ATX was superior to placebo in the 1.2 and 1.8 mg/kg/day dosing in all patients. For the PM patients the magnitude of the effect was greater at these doses compared to NMs (p<0.05) |
| 11854152 | NA | NA | A) 2 human microsomes samples containing full complement of CYPs; B) 2 human microsomes samples CYP2D6-deficient | In-vitro | NA | Enzyme kinetic analyses of 4-OH ATX formation: A) CLint (Vmax/Km) are 50 and 155 B) CLint (Vmax/Km) are 0.1 and 0.3 |
| 12485958 | 4 NM; 3 PM | NA (PM alleles genotyped) | 7 | USA | Twice a day 20mg for 5 days | Decreased rate of 4-OH ATX formation in PM with slower mean apparent ATX clearance (25% of NM) |
| 17242628 | 559 NM; 30 PM | NA (*3, *4, *5, *6, *7, *8) were genotyped and patients were grouped PM being homozygous for one of these or a combination of 2 no function alleles; all other patients grouped as NM) | 589 children and adolescents with ADHD | African (14.8%), Asian (0.7%), White (69.8%), Hispanic (10.1%), other | NM: mean dose 1.37 mg/kg/day; PM: mean dose 1.28 mg/kg/day (allowed up to a maximum of 1.8mg/kg daily) | Greater improvement in PM vs. NM patients; ADHDRS p=0.002, CGI-S p=0.052, % responders (defined as greater than 25% reduction from baseline) p=0.033 |
| 17242628 | 2563 NM; 171 PM | NA (*3, *4, *5, *6, *7, *8 were genotyped and patients were grouped PM being homozygous for one of these or a combination of 2 no function alleles; all other patients grouped as NM) | 2734 children and adolescents with ADHD, all studies combined (unclear how many per studied vital sign) | African, Asian, White, Hispanic, other | ATX dose >1.2 mg/kg/day | Greater increase in pulse (p<0.001) and diastolic blood pressure (p=0.012) in PM compared to NM, non-significantly increased weight gain for NM compared to PM (p=0.088), no difference in effects on QT interval |
| 17242628 | 313NM; 25 PM | NA (*3, *4, *5, *6, *7, *8 were genotyped and patients were grouped PM being homozygous for one of these or a combination of 2 no function alleles; all other patients grouped as NM) | 338 children and adolescents with ADHD | African, Asian, White, Hispanic, other | 1.0 mg/kg/day (divided in twice daily) | Mean peak concentration of ATX 5 times higher in PM compared to NM |
| 20691935 | NA | *1/ *4, *5/ *41 | 100 children with ADHD | Netherlands | 0.6 to 1.8 mg/kg/day based on response | From 100 patients 10 met the criteria of either late onset of effect (>9 weeks) or ADR and were genotyped for CYP2D6 (*2, *3, *4, *5, *6, *9, *10, *41) and CYP2C19*2. Patients with *1/ *4 (3) and *5/ *41 (1) discontinued treatment due to ADRs at 40mg and 80mg ATX, respectively. Patients with *1/ *4 (1), *2/*4, *2/*10 (1), and *1/*9 (1) showed good response and tolerance after a dose reduction from 60 to 40 mg (*1/*4, *2/*4 and *2/*10) or from 40 to 25 mg (*1/*9) |
| 19387424 | NA | NA (*3, *4, *5, *6, *7, *8 were genotyped and patients were grouped PM being homozygous for one of these or a combination of 2 no function alleles; all other patients grouped as NM) | Two trials 160 and 105 children with ADHD, analyzed separate and combined | Mixed and sub-analysis in Caucasian only | 0.5¿mg/kg/day to 1.8¿mg/kg per day | No significant difference in the treatment effect, as measured by ADHDRS end point values (p>0.05) is found after 6 weeks of treatment using the ADHDRS and CGI-S scores to determine response |
| 25919121 | UMs (>2 functional alleles) n=67, NM (2 normal function alleles) n=972, IM (normal + decreased n=79, normal + no n=670, two decreased n=6), PM (two no function alleles) n=117 | *1/*1xN, *1/*1, *1/*10, *1/*17, *1/*3, *1/*4, *1/*5, *1/*6, *1/*7, *10/*10, *10/*17, *17/*17, *3/*3, *3/*4, *3/*5, *3/*6, *4/*4, *4/*4xN, *4/*5, *4/*6, *5/*5, *4xN/*5 | 1967 adults with ADHD | Mixed | 40 mg/day for 2 weeks than increased to 80mg/day | Safety and tolerance is assessed by the frequency of reported treatment-emergent ADRs. PM compared to none-PM had a significant higher frequency of dry mouth, erectile dysfunction, hyperhidrosis, insomnia and urinary retention. No significant differences between normal/ultrarapid and intermediate metabolizers were found for treatment-emergent adverse events. |
| 26660002 | NM2 two normal function alleles n=8, NM1 one normal function allele n=8, IM n=3, PM n=4 | *1/*2xN, *1/*1, *1/*2, *2/*4, *1/*3, *1/*4, *2/*5, *2/*4, *9/*29, *10/*41, *5/*17, *4/*4, *4/*4xN, *4/*9 | 23 children and adolescent with ADHD | Mixed | Single dose study with average dose of 0.43 +/-0.07 mg/kg | Dose-corrected ATX systemic exposure varied 29.6-fold across subjects, ranging from 4.4±2.7 µM*h in NM2 to 5.8±1.7 µM*h, 16.3±2.9 µM*h and 50.2±7.3 µM*h in EM1, IM and PM, respectively (p<0.0001). No difference in pulse increase is seen between the metabolizer groups. |
| 17470523 | NA | *10, *17 | In-vitro | NA | NA | Microsomal preparation from insect cells expressing *1, *10, *17. Formation of 4OH-ATX from ATX was measured. ATX clearance was 8.58% and 21.9% of *1 in *10 and *17, respectively. But compared to other 2D6 substrates clearance for *10 and *17 was quite high |
| 17610534 | NA | *10/*10 (9), *1/*10 and *1/*1 (7) | 16 healthy adults | China | ATX 40 mg once daily for 3 days followed by ATX 80 mg for 7 days | Mean clearance was about 50% lower in *10/*10 compared to *1/*10 and *1/*1; doses were well tolerated in all participants |
| 21543662 | NA | *10/*10, *1/*10 and *1/*1, *1/*2 | 49 healthy adults | Japan | ATX single-stepped dosing and multiple doses (40 or 60 mg twice daily) for 7 days | *10/*10 subjects had 2.1- to 2.2-fold and 1.8-fold higher AUC values relative to the CYP2D6*1/*1 and *1/*2 subjects and the CYP2D6*1/*10 and *2/*10 subjects; no differences in tolerance |
| 26254792 | NA | *1/*1 (22), *1/*10 (22), *10/*10 (18) | 62 healthy adults | Korea | Single dose of 12, 16, 30, 40 mg ATX | Higher plasma concentrations (Cmax and AUC) for *10 carrier and reduced clearance |
| 26666748 | NA | NA | In-vitro recombinant expressed CYP2D6 in insect cells | NA | NA | *2 + *10 + *87 + *88 + *90 + *91 + *93 + *95 + *97 showed decreased intrinsic clearance of ATX compared to wild type, *92 and *96 activity was too weak to result in measurable 4-OH ATX formation. Study does not report the exact variation introduced to created the star alleles; e.g. *2 |
ADHD: Attention Deficit – Hyperactivity Disorder; ADHDRS: Attention Deficit – Hyperactivity Disorder Rating Scale; ATX: atomoxetine; AUC: area under the plasma concentration-time curve NM: normal (former extensive) metabolizer; PM: poor metabolizer; NA: not available (not reported)
Reactions & interactions (17)
-
Biochemical Reaction
atomoxetine → 4'-hydroxy atomoxetine
-
Biochemical Reaction
4'-hydroxy atomoxetine → 4-hydroxyatomoxetine-O-glucuronide
-
Biochemical Reaction
atomoxetine → N-desmethyl atomoxetine
-
Biochemical Reaction
atomoxetine → 2-hydroxymethyl atomoxetine
-
Biochemical Reaction
N-desmethyl-4-hydroxyatomoxetine → N-desmethyl-4-hydroxyatomoxetine glucuronide
-
Biochemical Reaction
atomoxetine → 4'-hydroxy atomoxetine
-
Biochemical Reaction
N-desmethyl atomoxetine → N-desmethyl-4-hydroxyatomoxetine
-
Catalysis
CYP2D6 → Biochemical Reaction
-
Catalysis
CYP2C19 → Biochemical Reaction
-
Catalysis
CYP2B6 → Biochemical Reaction
-
Catalysis
CYP2D6 → Biochemical Reaction
-
Catalysis
CYP2C19 → Biochemical Reaction
-
Catalysis
CYP2E1 → Biochemical Reaction
-
Catalysis
CYP3A4 → Biochemical Reaction
-
Catalysis
CYP1A2 → Biochemical Reaction
-
Catalysis
CYP2B6 → Biochemical Reaction
-
Catalysis
CYP2D6 → Biochemical Reaction
Edit history (2)
- 2016-10-17 Create
- 2025-07-17 Update changed link