About this pathway
Introduction
Sirolimus, also known as rapamycin, is a macrolide compound used to inhibit cellular proliferation [Article:19362662]. It is primarily used as an immunosuppressant for patients undergoing organ transplantation, though it can also be used as a chemotherapeutic agent [Article:27187382]. The drug is unique from the calcineurin inhibitors tacrolimus and cyclosporine, two mainstay immunosuppressants, in its targeting of mammalian target of rapamycin (mTOR) [Articles:17151193, 26501229]. mTOR coordinates cell growth and proliferation and its signaling pathway is implicated in the development of conditions such as cancer, neurological diseases, obesity, and genetic disorders [Articles:22500797, 24508508]. Given the involvement of mTOR in various critical biological functions, sirolimus may have many treatment applications beyond organ transplantation. However, the drug is known to display large interpatient variation in its pharmacokinetic parameters [Articles:11907172, 15385826], and is associated with a variety of adverse effects [Article:19362662]. The wide variation in pharmacokinetic parameters may be partially due to genetic changes in the proteins involved in sirolimus metabolism. This review will provide an overview of the literature on the pharmacokinetics, pharmacodynamics, and pharmacogenetics of sirolimus. A particular emphasis will be given to pharmacogenetics, as developments in this area may provide a way to optimize dosing.
Pharmacokinetics
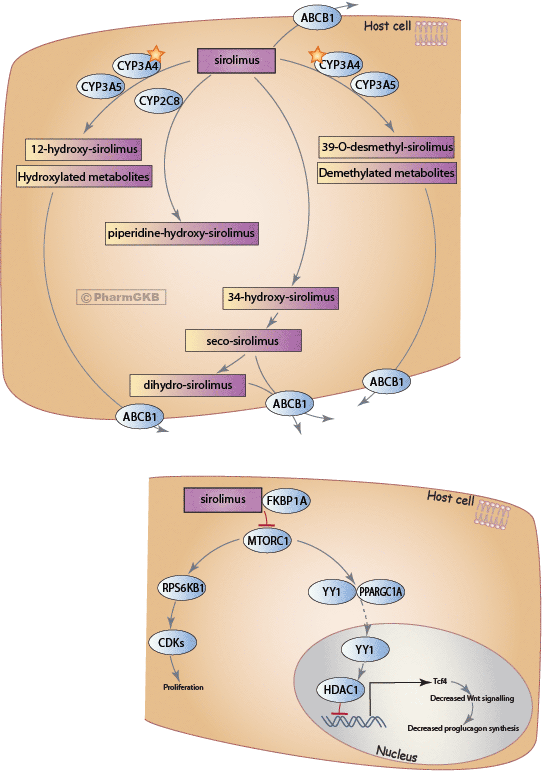
A schematic representation of sirolimus pharmacokinetics and pharmacodynamics is provided in the figure above. Sirolimus has a low average bioavailability (~20%), likely due to extensive metabolism in both the intestine and the liver [Articles:8937863, 11907172]. Within the intestine and liver, sirolimus is metabolized into various demethylated and hydroxylated products [Article:15385826]; a degradation product, 34-hydroxy sirolimus, is also formed [Article:8937863], as well as a metabolite known as piperidine-hydroxy sirolimus [Articles:11266932, 18482220]. Specific sirolimus metabolite patterns are not well-defined, though several major metabolites have been identified, including 39-O-demethyl sirolimus, and 12-hydroxy sirolimus, and 34-hydroxy sirolimus [Articles:18482220, 8937863]. 39-O-demethyl sirolimus is known to retain approximately 10% of the immunosuppressive activity of sirolimus; 12-hydroxy sirolimus is known to retain 7% [Articles:18482220, 1352208]. 34-hydroxy sirolimus is further metabolized in seco-sirolimus, and then into a hydrogenated metabolite [Articles:11907172, 10833025, 15385825].
CYP3A4 is the main enzyme involved in sirolimus metabolism, though CYP3A5 and CYP2C8 also play a role [Articles:11266932, 14569063]. CYP2C8 has a strong preference for the metabolism of the piperidine ring in the sirolimus structure, which creates the metabolite piperidine-hydroxy sirolimus [Article:11266932]. Filler et al. note that piperidine hydroxylation is rarely seen in adults (unpublished data), but in pediatric patients, it was formed at a considerable rate [Article:18482220]. The enzyme or enzymes involved in the metabolism of 34-hydroxy sirolimus into seco-sirolimus and its hydrogenated metabolite are not known [Articles:11907172, 10833025, 15385825]. Sirolimus and its metabolites are believed to be substrates for ABCB1 transport [Articles:14569063, 11907172, 15385826].
Pharmacodynamics
The mammalian target of rapamycin (mTOR) functions as two separate signaling complexes, mTORC1 and mTORC2, and is pivotal in regulating cell growth, proliferation, metabolism, and angiogenesis, amongst a bevy of other functions [Articles:12408816, 12901945, 14536067, 7569949, 8387896]. After entering cells, sirolimus forms an inhibitory complex with FKPB12 (encoded by the FKBP1A gene) that targets mTORC1, inhibiting downstream effects, which explains its potent immunosuppressive and antiproliferative properties [Articles:7539137, 8662507]. For example, sirolimus inhibits mTORC1 after entering T lymphocytes, which enhances mTORC2 activity and shifts the balance between these mTOR complexes, suppressing the pro-inflammatory cytokine milieu [Articles:12150926, 23913957, 24683191]. Furthermore, the cellular energy balance regulates mTORC1 via ATP-sensitive AMPK, and if activated will initiate the phosphorylation cascade involving p70-S6 kinase (encoded by the RPS6KB1 gene) and 4E-BP1 (encoded by the EIF4EBP1 gene), increasing ribosome activity and translation that regulates cancerous characteristics like cell growth, survival, proliferation, and motility [Articles:12150925, 20812900].
Sirolimus is not without its side-effects. In the cytosol, mTORC1 heterodimerizes with YY1 and PGC-1α to form a transcriptional complex that undergoes nuclear translocation to activate mitochondrial gene expression [Article:18046414]. However, this transcriptional complex may also recruit HDAC to promoters like that of TCF7L2, a gene encoding the Tcf4 transcription factor that facilitates expression of Wnt target genes causing decreased proglucagon synthesis [Articles:17206141, 18599616, 17640524, 19439614]. Hence, sirolimus inhibition of mTORC1 releases the inhibition of TCF7L2 expression, which contributes to perturbations to glucose homeostasis and new-onset diabetes after transplantation (NODAT) [Articles:18385422, 17671651]. This section briefly covers the immense scope of mTOR pathways; however, this summary focuses on variants in the human genome and their effect on sirolimus pharmacokinetics and treatment.
Pharmacogenomics
Since CYP3A4 and CYP3A5 are the main enzymes involved in sirolimus metabolism, most pharmacogenetics studies on sirolimus have focused on variants within these genes, particularly on CYP3A5. However, some associations have been seen for variants within the ABCB1 gene, which is believed to be involved in sirolimus transportation and cholesterol and lipid homeostasis. Additionally, one study also examined the TCF7L2 gene, which is involved in the pharmacodynamics of sirolimus.
ABCB1
The ABCB1 rs1045642 A allele appears to be detrimental for cholesterol homeostasis in patients receiving sirolimus after renal transplantation: individuals with the AA or AG genotype had elevated levels of total and low-density lipoprotein (LDL) cholesterol as compared to those with the GG genotype [Article:23073467]. Within the same study, the ABCB1 rs1128503 G allele was associated with decreased triglyceride levels as compared to those patients with the AA genotype [Article:23073467]. ABCB1 is believed to be involved in the transport of sirolimus and its metabolites, but it is also known to be involved in cholesterol and lipid homeostasis, providing a possible explanation for the association with cholesterol and triglyceride levels [Article:23073467]. Additionally, Sam et al. found that patients with the rs1045642 A allele also had higher sirolimus dose-adjusted trough concentrations as compared to patients with the GG genotype [Article:22094953]. Lastly, Khaled et al. found that hematopoietic stem cell transplant patients who carried the ABCB1 rs2032582 A allele had higher sirolimus concentrations as compared to non-A allele carriers [Article:26325438]. However, some studies have found no association between ABCB1 variants and sirolimus concentrations [Articles:15707415, 17941052, 26543771].
CYP3A4
Anglicheau et al. found that kidney transplant patients carrying the CYP3A4 rs2740574 C allele (also known as CYP3A4*1B) required significantly higher doses of sirolimus to achieve adequate blood concentrations as compared to those with the TT (or *1/*1) genotype [Article:15707415]. However, it is important to note that this variant is in strong linkage disequilibrium with CYP3A5 rs776746 (discussed below) [Article:15707415]. An in vitro study found that the CYP3A4 rs35599367 T allele (also known as CYP3A4*22) was associated with decreased metabolism of sirolimus [Article:23974086]. However, in kidney transplant patients, no association was found with sirolimus dose or concentrations [Article:23974086]. Additionally, this CYP3A4 variant was also in strong LD with rs776746 [Article:23974086].
CYP3A5
Similar to CYP3A4 variants, kidney transplant patients with the CYP3A5 rs776746 CC (also known as CYP3A5*3/*3 or a non-expressor) genotype may also require lower daily doses of sirolimus to obtain optimal trough blood concentrations as opposed to those with the CT or TT (*1/*1 or *1/*3, expressor) genotypes [Articles:15707415, 16815317, 17941052, 26543771]. One study has found no association between CYP3A5 rs776746 and sirolimus metabolism [Article:23974086].
TCF7L2
TCF7L2 encodes Tcf4, a high mobility group box-containing transcription factor. Tcf4 plays a role in expressing Wnt target genes, which inhibit proglucagon synthesis in enteroendocrine cells, thereby affecting blood glucose homeostasis [Articles:17206141, 18599616]. Patients who were taking cyclosporine, tacrolimus or an mTOR inhibitor and who carried the rs7903146 T allele had an increased risk for new-onset diabetes after transplantation (NODAT) [Article:19713311]. The rs7903146 T allele is also associated with the development of type 2 diabetes independently of the use of calcineurin or mTOR inhibitors [Articles:16415884, 17671651], and sirolimus has been shown to be associated with NODAT independently of rs7903146 [Article:18694475]; sirolimus has also been shown to cause insulin resistance in Sprague Dawley rats [Article:16926589]. Therefore, it will be useful in future studies to pinpoint the pharmacogenetic relationship between rs7903146, sirolimus, and the development of type 2 diabetes. One hypothesis by Tyler et al. is that mTORC2 facilitates its transcriptional control via Tcf4 [Article:19439614], which is further supported by mTORC1 being able to modulate and heterodimerize with the transcription factor YY1 (Ying Yang 1), which recruits histone deacetylase (HDAC) to the promoter of TCF7L2 in oligodendrocyte differentiation [Articles:18046414, 17640524]. Therefore, when mTOR is inhibited by sirolimus, this may lead to increased Tcf4 levels. Indeed, the T allele is associated with overexpression of TCF7L2 that impairs the enteroinsular axis, affecting insulin secretion, incretin effects, and increased rate of hepatic glucose production [Article:17671651].
Conclusions
While studies on the pharmacogenetics of sirolimus are currently limited, a number of studies have found significant associations with its metabolism and adverse effects. Given the range of possible therapeutic applications for the drug, it is important that further studies are undertaken on its pharmacogenetics, in order to ensure correct dosing and avoid harmful effects.
Reactions & interactions (40)
-
Activation
MTORC1 → RPS6KB1
-
Activation
YY1 → HDAC1
-
Activation
RPS6KB1 → CDKs
-
Activation
CDKs → Proliferation
-
Activation
TCF7L2 → Regulation of Wnt signaling pathway
-
Biochemical Reaction
sirolimus → 12-hydroxy-sirolimus
-
Biochemical Reaction
sirolimus → hydroxylated sirolimus metabolites
-
Biochemical Reaction
sirolimus → demethylated sirolimus metabolites
-
Biochemical Reaction
MTORC1 + YY1-PPARGC1A → YY1
-
Biochemical Reaction
sirolimus → 39-o-desmethyl sirolimus
-
Biochemical Reaction
34-hydroxy-sirolimus → seco-sirolimus
-
Biochemical Reaction
seco-sirolimus → dihydro-sirolimus
-
Biochemical Reaction
sirolimus → piperidine-hydroxy-sirolimus
-
Biochemical Reaction
sirolimus → 34-hydroxy-sirolimus
-
Catalysis
CYP3A5 → Biochemical Reaction
-
Catalysis
CYP3A4 → Biochemical Reaction
-
Catalysis
CYP3A4 → Biochemical Reaction
-
Catalysis
CYP3A5 → Biochemical Reaction
-
Catalysis
ABCB1 → Transport
-
Catalysis
CYP3A4 → Biochemical Reaction
-
Catalysis
CYP3A5 → Biochemical Reaction
-
Catalysis
CYP3A5 → Biochemical Reaction
-
Catalysis
CYP3A4 → Biochemical Reaction
-
Catalysis
CYP2C8 → Biochemical Reaction
-
Catalysis
ABCB1 → Transport
-
Catalysis
ABCB1 → Transport
-
Catalysis
ABCB1 → Transport
-
Catalysis
ABCB1 → Transport
-
Catalysis
ABCB1 → Transport
-
Catalysis
ABCB1 → Transport
-
Inhibition
sirolimus-FKBP1A → MTORC1
-
Inhibition
HDAC1 → TCF7L2
-
Template Reaction
TCF7L2 → TCF7L2
-
Transport
demethylated sirolimus metabolites → demethylated sirolimus metabolites
-
Transport
sirolimus → sirolimus
-
Transport
12-hydroxy-sirolimus → 12-hydroxy-sirolimus
-
Transport
dihydro-sirolimus → dihydro-sirolimus
-
Transport
seco-sirolimus → seco-sirolimus
-
Transport
39-o-desmethyl sirolimus → 39-o-desmethyl sirolimus
-
Transport
hydroxylated sirolimus metabolites → hydroxylated sirolimus metabolites
Edit history (1)
- 2017-06-09 Create