About this pathway
Introduction
Sertraline, a selective serotonin reuptake inhibitor (SSRI), is commonly prescribed to treat several psychiatric disorders including major depressive disorder, panic, generalized and social anxiety disorders as well as obsessive-compulsive disorder (OCD). It has similar efficacy to other SSRIs and is considered to cause fewer side effects than some antidepressants, such as tricyclic antidepressants [Articles:8131293, 20393946]. However, sertraline-induced adverse events such as reversible hepatic injury and Stevens Johnson Syndrome/toxic epidermal necrolysis (SJS/TEN) have been reported [Articles:17805350, 18958618]. Sertraline is a secondary amine with two chiral centers [Articles:1431018, 10674711, 20953053, 29399539]. The potent cis-(1S,4S) enantiomer is used as an antidepressant in either a tablet or an oral solution [Articles:6310078, 1431018], although the (1R,4R) enantiomer also inhibits serotonin reuptake [Article:6310078].
Pharmacokinetics
Sertraline is slowly absorbed, with peak concentrations (Cmax) occurring at 4-10 hours following ingestion, and has a half-life of 24-32 hours in children, adolescents and adults [Articles:2949057, 3624397, 8941024, 9549959, 11452243, 12218424, 16438795, 18397687, 22011692, 29723928]. The therapeutic concentration range for sertraline has not been well established, but has been proposed to be 10-150 ng/mL [Article:21969060]. Concentrations below 10 ng/mL are proposed to have reduced efficacy, whereas concentrations above 150 ng/mL may increase the risk of toxicity. Chronopharmacokinetic studies suggest that the time of day that sertraline is administered does not influence the pharmacokinetic parameters [Article:9068936]. Taking sertraline with food can increase the Cmax by 25%, but plasma concentrations and area under the curve (AUC) between fasted and nonfasted groups 12 hours post-dose are comparable [Article:9068936].
Desmethylsertraline, the active metabolite of sertraline, has a half-life of 56-120 hours and reaches peak plasma concentrations 8-10 hours following administration [Articles:8941024, 9068932, 15252820, 19109078]. Serum desmethylsertraline and sertraline concentrations are correlated, although desmethylsertraline concentrations are generally higher than sertraline concentrations [Articles:8131293, 10942186].
There is a large interindividual variability in plasma concentrations between patients taking the same dose of sertraline, which may be partially due to variable expression of CYP3A4, discussed in the Metabolism section below [Articles:8131293, 10674711] and genetic variation in CYP2C19, discussed in the Pharmacogenomics section [Article:18677622]. This variability contributes to the weak relationship between the dose and plasma sertraline concentrations [Articles:10942186, 22011692]. Although some studies have found a relationship between serum concentrations of sertraline and the magnitude of clinical effect on patients [Article:10823294], other research has failed to replicate this association [Articles:15252820, 23318280].
Pharmacokinetics in special patient populations
Age may influence sertraline pharmacokinetics with elderly patients having increased serum concentrations and concentration/dose (C/D) ratios of sertraline and desmethylsertraline, compared to younger patients [Articles:10942186, 18677622]. However, not all studies have observed significant relationships between age and plasma sertraline concentrations [Articles:9068932, 15252820, 23318280]. Relative to adults, children (age 6-12 years) and adolescents (13-17 years) have reduced AUCs and Cmax, when plasma sertraline concentrations were adjusted for weight. However, Cmax and AUC vary considerably in pediatric pharmacokinetic studies of sertraline and some suggest that pharmacokinetic differences observed between children and adolescents are attributable to differences in body weight rather than age [Article:9549959].
Patients with cirrhosis have a significantly increased exposure to sertraline compared to patients with no hepatic impairment. This results from an increased Cmax, half-life and AUC of sertraline [Article:8877033] and reduced doses are recommended in patients with liver impairment . Sertraline AUC and Cmax are also increased in patients who have undergone roux-en-Y gastric bypass, suggesting that the absorption of sertraline is affected by the procedure [Article:21256091]. Renal impairment does not significantly affect sertraline pharmacokinetics.
In pregnant women, sertraline metabolism may be increased, which results in the potential need for dose increases during pregnancy. [Articles:19011433, 18426260]. Due to their high lipophilicity, sertraline (log Poct = 4.30) and desmethylsertraline can be detected in breast milk and in the plasma of breastfed infants of sertraline-treated mothers. However, these levels rarely exceeded 8ng/ml, with desmethylsertraline detected at slightly higher concentrations and more consistently across infants than sertraline [Articles:9108810, 9286185, 9643617, 9585724, 11531744, 11578995, 11483479, 16848750, 28511118]. Sertraline has a negligible effect on serotonin transport in breastfed infants [Article:11578995].
Transport, metabolism and excretion
Sertraline is highly protein-bound in the blood (98%) and binds to human serum albumin with a high affinity via hydrophobic interactions and hydrogen bonding [Article:26471709]. In an in vitro model of the blood-brain barrier using rodent cells, lipophilic sertraline molecules easily crossed the barrier [Article:25118670]. However, the pharmacokinetics of sertraline vary considerably across species and caution must be used in extrapolating results of studies in lower animals to humans [Article:2573498]. Additionally, both sertraline and desmethylsertraline are substrates of the transporter p-glycoprotein, encoded by ABCB1, and bind with high affinity [Article:18239278]. Sertraline can also inhibit p-glycoprotein, but this inhibition is not thought to have clinical effects [Articles:12649369, 23468867].
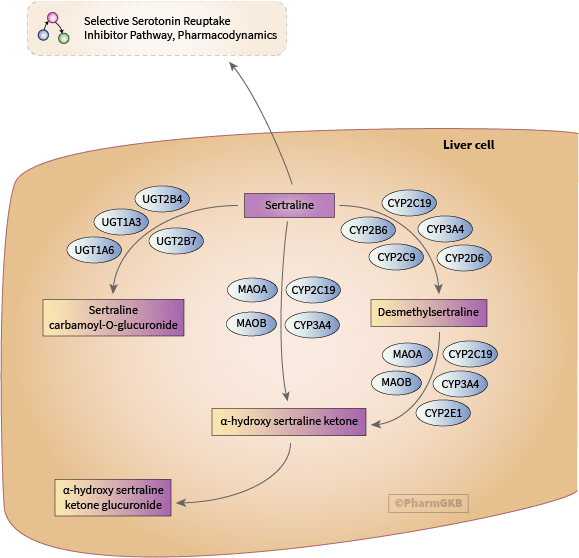
The main route of sertraline clearance is hepatic metabolism, as shown in the figure above [Articles:7990446, 10674711]. The vast majority of research concerning sertraline metabolism has focused on the demethylation of sertraline to form desmethylsertraline, the only active sertraline metabolite [Article:10379420]. This reaction is mediated by multiple cytochrome P450 (CYP) enzymes [Articles:10587282, 10674711].
No individual CYP enzyme is thought to mediate more than 25-35% of sertraline’s metabolism to desmethylsertraline [Articles:10587282, 10383917]. At high in vitro sertraline concentrations, metabolism is primarily driven by CYP2C9, CYP3A4 and CYP2C19, with CYP2D6 and CYP2B6 making minor contributions [Articles:10587282, 10510155, 15547048]. However, at lower concentrations, CYP2D6 and CYP2B6 play a more prominent role in desmethylsertraline formation, while CYP3A4 has a smaller role [Articles:10383917, 15547048, 28737446].
In vivo, inhibition of CYP3A4 increases serum sertraline concentrations [Articles:10890261, 19172438] while possible CYP3A4 induction by carbamazepine decreases sertraline concentrations [Articles:10937612, 11936714]. Inhibition of CYP2C19 (e.g. by the proton pump inhibitor esomeprazole) increases sertraline C/D ratios. Readers should note that other proton pump inhibitors (e.g., omeprazole, lansoprazole and pantoprazole) do not appear to affect sertraline pharmacokinetics [Article:24887634].
In addition to metabolism by CYP enzymes, sertraline and desmethylsertraline can be deaminated to α-hydroxy sertraline ketone by CYP3A4, CYP2C19, monoamine oxidase A (MAO-A) and monoamine oxidase B (MAO-B) [Article:15547048]. Desmethylsertraline can also be deaminated by CYP2E1 [Article:15547048]. α-hydroxy sertraline ketone is subsequently glucuronidated [Article:11420570]. Additionally, sertraline can be glucuronidated via a carbamic acid intermediate to sertraline carbamoyl-O-glucuronide by UGT1A3, UGT1A6, UGT2B4 and UGT2B7 [Articles:2566471, 15547048].
Only low concentrations of unchanged sertraline can be recovered from urine, indicating that sertraline is extensively metabolized to its major excretory metabolite, α-hydroxy sertraline, prior to excretion [Articles:7990446, 15547048].
Drug-drug interactions involving sertraline
The fact that sertraline interacts with a number of CYP enzymes means that the metabolism of other drugs can be affected by the presence of sertraline. Sertraline reduces the clearance and potentiates the effects of imipramine and desipramine, due to inhibition of CYP2D6 [Articles:8214190, 8317590, 8195463, 9241008, 9284850]. In the case of imipramine, it is thought that inhibition of CYP2D6 by sertraline may increase the conversion of imipramine to desipramine [Article:9284850]. In vitro data indicate that sertraline also moderately inhibits the CYP2D6-mediated metabolism of timolol, sparteine and propafenone [Articles:1389951, 10917404, 19912165]. However, other work has found sertraline to only be a weak CYP2D6 inhibitor [Articles:10950472, 9681670, 9472843, 12173784, 11910262, 15257068, 17224709], concurring with the findings of the US Food and Drug Administration (FDA) (see Table 3-2 at https://www.fda.gov/drugs/drug-interactions-labeling/drug-development-and-drug-interactions-table-substrates-inhibitors-and-inducers), or to have no significant inhibitory effect at all [Articles:10211917, 10631623]. Some in vivo data suggest that weak CYP2D6 inhibition (AUC fold-change 1.25-2) occurs after achievement of steady-state concentrations while insignificant inhibitory effects are typically seen prior to steady state [Articles:8195463, 9241008, 9284850, 17224709].
Research on the inhibitory effect of sertraline on CYP2C9 indicates that the degree of inhibition may be substrate specific. Sertraline is a moderate inhibitor of phenytoin hydroxylation in vitro and can increase plasma phenytoin concentrations in patients [Articles:10950473, 9384467, 11255075]. However, sertraline only has a weak inhibitory effect on the metabolism of warfarin and tolbutamide [Articles:9068934, 9068933, 10192756].
Two studies have investigated sertraline’s ability to inhibit CYP2C19. One study found that sertraline could inhibit S-mephenytoin 4’hydroxylation by 73.3% [Article:8703653] while Wang et al. determined that sertraline was a weak inhibitor of CYP2C19 [Article:21692664]. The inhibitory potency of sertraline may be allele-specific: it inhibits the CYP2C19*8, *9, *13, *14, *16, and *19 alleles to a lesser degree than the *1 allele, but more strongly inhibits the *11 allele than the *1 allele by assessment of IC50 values [Article:21692664]. The mechanism which underlies these allele-specific inhibitory effects of sertraline is currently unclear.
Sertraline may act as a CYP3A4/5 inhibitor [Articles:7946933, 8531073, 15257068, 23929629], although several studies have failed to observe this [Articles:9068935, 10770452, 11001249, 11910261, 14709940, 25971243, 27060853]. Interestingly, in one study, sertraline increased the cytotoxicity of carbamazepine by increasing CYP3A4-mediated production of reactive carbamazepine metabolites [Article:25656284]. Additionally, desmethylsertraline may inhibit CYP3A4/5 but to a lesser extent than sertraline [Article:23929629]. Sertraline does not inhibit CYP1A2 [Articles:9472843, 11477325, 25971243, 27060853] but may act as a CYP1A2 inducer [Article:10950477]. There is some evidence that sertraline inhibits CYP2B6 and impacts the pharmacokinetics of efavirenz and methadone, which are both CYP2B6 substrates [Articles:10914294, 19074527, 26643342]. This inhibition is reduced when the increased-function CYP2B6*4 allele or decreased-function CYP2B6*6 allele are present [Article:19074527].
In addition to inhibiting cytochrome P450 enzymes, sertraline interacts with several other enzymes and transporters [Articles:9627209, 10557352, 23962042]. Cases of serotonin syndrome in patients taking sertraline and a concomitant serotonergic drug, such as tramadol or clozapine, have been reported and the potential for sertraline to contribute to serotonin syndrome is acknowledged on the drug label [Articles:9034418, 15190240, 26161840]. However, such cases are extremely rare, and questions have been raised as to whether prescribing actions should be changed to account for the low possibility of a patient developing serotonin syndrome. A retrospective study of 19,017 patients prescribed both an SSRI and a triptan, a combination considered by the FDA to potentially increase the risk of serotonin syndrome, found only seven cases of serotonin syndrome [Article:29482205].
Pharmacodynamics
Sertraline is prescribed for its property as an inhibitor of the serotonin transporter SLC6A4. The pharmacodynamics of SSRIs have been covered in the Selective Serotonin Reuptake Inhibitor Pathway, Pharmacodynamics [Article:19741567]. Briefly, inhibition of SLC6A4 by sertraline is thought to potentiate the synaptic effects of serotonin and enhance signaling by the serotonin receptors. However, sertraline also inhibits transport of sodium, norepinephrine reuptake, dopamine reuptake as well as glutamate and GABA cycling in rodent and human neurons [Articles:6310078, 9400006, 22288826].
Although desmethylsertraline is an active metabolite of sertraline, it has no significant effect on serotonin reuptake [Article:8924190] as its potency as a serotonin reuptake inhibitor is approximately 20-fold less than that of sertraline [Articles:6310078, 7535937]. As such, desmethylsertraline is not considered to exert a notable clinical effect in sertraline-treated patients. Similar to sertraline, desmethylsertraline weakly inhibits the norepinephrine transporter [Article:7535937].
Pharmacogenomics
CYP2C19 variants appear to have the greatest impact on sertraline pharmacokinetics. Patients who are CYP2C19 poor metabolizers (PMs), or those carrying the *2 or *3 no function alleles, have a significantly slower rate of desmethylsertraline formation compared to CYP2C19 normal metabolizers (NMs) and consequently have an increased exposure to the pharmacologically active parent compound [Articles:10510155, 11452243, 15168101, 18677622]. Sertraline dose extrapolations based on pharmacokinetic parameters among CYP2C19 phenotypes suggest a 50% dose reduction may be needed for poor metabolizers [Article:22565785]. A recent study found that the number of CYP2C19 no function alleles influenced the rate of titration of sertraline in a retrospective cohort of children and adolescents with anxiety and depressive disorders [Article:31066578]. While the relationship between CYP2C19 increased or no function alleles and sertraline exposure and response is still being elucidated [Articles:23545896, 26830411], the increased function CYP2C19*17 allele has not been observed to greatly affect sertraline plasma concentrations [Article:18677622].
Several studies have found no significant effect of CYP2D6 and CYP2C9 alleles on sertraline pharmacokinetics or patient response [Articles:8941024, 10510155, 23545896] and research into the effect of genetic variants on SSRIs did not find a significant impact of CYP2D6*4 on sertraline dose and tolerability [Article:18070221]. However, analysis of a single patient with the CYP2D6 ultrarapid metabolizer (UM) phenotype and a single patient with the CYP2D6 PM phenotype found a reduction in sertraline plasma concentrations in both patients compared to the median concentrations across the cohort [Article:15168101]. Given that these observations were made in individual patients, the influence of confounding factors, such as treatment adherence, cannot be excluded. This is particularly true in the case of the CYP2D6 PM patient as they presented with side effects at the first visit and had a subsequent change in diagnoses. Despite its unclear contribution to sertraline metabolism, the *6 and *9 alleles of CYP2B6 have been shown to decrease the rate of desmethylsertraline formation in one study [Article:26830411].
The SNPs rs1045642, rs2032583, rs2032582, rs2235040, rs2235015, and rs9282564 in ABCB1 are associated with side effects and time to remission in patients taking sertraline [Article:25487678]. However, the mechanism behind this observation is still unclear and is complicated by a study which found no effect of rs1045642 on sertraline clearance [Article:29723928].
Patients that are homozygous for the 5HTTLPR long allele in SLC6A4 have shown an improved response to sertraline compared to patients with one or two copies of the short allele [Articles:12955294, 21962566, 31066578]. However, not all studies have observed this effect [Articles:16580768, 18452396]. In addition, one study found no association between a variable number tandem repeat (VNTR) in SLC6A4 and sertraline response [Article:18452396]. An association between the deletion allele of rs1799752 in ACE and improved sertraline response has also been reported [Article:27262302]. The deletion allele has been linked to increased plasma levels of angiotensin-converting enzyme (ACE) [Article:1976655] and may affect the response of the renin angiotensin system to antidepressant therapy.
The GG genotype of rs45476395 in GNB3 has been associated with an improved response to sertraline in patients with major depressive disorder (MDD) [Article:30324302]. However, the same study did not find an association between rs5441 in GNB3 and response to sertraline. As GNB3 encodes the G protein β3 subunit, the authors suggest that variants in this gene may affect signaling cascades involved in MDD or in the physiological response to sertraline.
In a study of Australian and Malaysian patients, Hong Ng et al. noted an association between a patient’s ethnic background and their sertraline plasma levels and treatment response. However, the authors only analyzed associations between ethnicity and sertraline pharmacokinetics and response and did not attempt to determine which pharmacogenetic variants may subtend these differences [Article:16421459].
There are limited data on the pharmacogenetics underlying sertraline-related side effects. HLA-A*33:01 has been identified as a risk factor for sertraline drug-induced liver injury [Article:28043905], but there is currently no information on which HLA alleles are involved in the onset of sertraline-induced SJS/TEN. A study of the HTR2A variants rs6311 and rs6313 did not find an association between either SNP and sertraline-induced nausea and vomiting [Article:30221791].
Pharmacogenomics of antidepressants
Sertraline has been included in a number of studies investigating the pharmacogenetics of antidepressants more generally. The A allele of rs2235040 and the C allele of rs2032583, both in ABCB1, have been associated with increased adverse effects, serotonergic side effects (e.g., diarrhea or nausea) and SSRI-related insomnia [Article:22641028]. However, another study failed to find an association between rs2032583 and SSRI side effects in addition to finding no association between rs2032583 or rs2235015 and SSRI dose/plasma concentrations [Article:26704739]. Similarly, variants in ABCB6 and ABCG1 have not been associated with SSRI response [Article:24192121].
Other research into genetic influences on antidepressant response have implicated a haplotype of rs6311, rs6313 and rs1928040 in HTR2A, rs6295 in HTR1A and rs495794 and rs153560 in _REEP5+ with response to antidepressants including sertraline [Articles:19937159, 19800133, 22795047]. Specifically, in one retrospective pediatric study of 249 sertraline-treated patients, HTR2A rs6313 and rs7997012 were associated with the dose at the time of response [Article:31066578]. HTR1A and HTR2A encode serotonin receptor proteins, while REEP5 encodes an accessory protein.
Clinical implementation
As a result of this research, clinical guidelines have been published concerning sertraline use in CYP2C19 PMs [Articles:16384813, 21412232, 25974703]. These include the Clinical Pharmacogenetic Implementation Consortium (CPIC) guideline which recommends that, due to the risk of increased side effects, clinicians treating CYP2C19 PMs may consider reducing the starting dose by 50% before titrating to response or selecting an alternative antidepressant not predominantly metabolized by CYP2C19 [Article:25974703]. The Royal Dutch Pharmacists Association - Pharmacogenetics Working Group (DPWG) also recommends using lower doses in patients who are CYP2C19 PMs [Article:21412232]. Both of these guidelines have been annotated on the ClinPGx website. Several institutions have implemented the CPIC and DPWG guidelines into clinical care for routine use or research projects [Articles:28749586, 30299306, 30058217].
Conclusion
While the in vivo metabolism of sertraline in humans has not been fully investigated, variants in a number of genes involved in the sertraline pharmacokinetics and pharmacodynamics appear to affect its metabolism and clinical response. Current clinical guidelines focus on the possible effect of CYP2C19 variants on sertraline but further research could provide evidence to justify the inclusion of variants in genes involved in drug transport and response in future guidelines.
Reactions & interactions (25)
-
Biochemical Reaction
sertraline → sertraline carbamoyl-O-glucuronide
-
Biochemical Reaction
desmethylsertraline → alpha-hydroxy sertraline ketone
-
Biochemical Reaction
sertraline → alpha-hydroxy sertraline ketone
-
Biochemical Reaction
sertraline → desmethylsertraline
-
Biochemical Reaction
alpha-hydroxy sertraline ketone → alpha-hydroxy sertraline ketone glucuronide
-
Catalysis
UGT2B4 → Biochemical Reaction
-
Catalysis
UGT1A6 → Biochemical Reaction
-
Catalysis
UGT1A3 → Biochemical Reaction
-
Catalysis
UGT2B7 → Biochemical Reaction
-
Catalysis
MAOB → Biochemical Reaction
-
Catalysis
CYP3A4 → Biochemical Reaction
-
Catalysis
MAOA → Biochemical Reaction
-
Catalysis
CYP2E1 → Biochemical Reaction
-
Catalysis
CYP2C19 → Biochemical Reaction
-
Catalysis
CYP3A4 → Biochemical Reaction
-
Catalysis
MAOA → Biochemical Reaction
-
Catalysis
MAOB → Biochemical Reaction
-
Catalysis
CYP2C19 → Biochemical Reaction
-
Catalysis
CYP2B6 → Biochemical Reaction
-
Catalysis
CYP2D6 → Biochemical Reaction
-
Catalysis
CYP2C19 → Biochemical Reaction
-
Catalysis
CYP2C9 → Biochemical Reaction
-
Catalysis
CYP3A4 → Biochemical Reaction
-
Leads To
sertraline → Selective Serotonin Reuptake Inhibitor Pathway, Pharmacodynamics
-
Transport
sertraline → sertraline
Edit history (4)
- 2018-10-30 Create
- 2019-11-04 Update Updated description to reflect reviewer corrections made to submitted manuscript
- 2020-01-16 Update Added sertraline pathway publication
- 2025-07-17 Update Replaced link in text to CYP3A (non-specific) with CYP3A4