About this pathway
Acetaminophen (N-acetyl-p-aminophenol, APAP, or paracetamol, PARA) is widely used for its analgesic and antipyretic properties in many over-the-counter formulations in both adults and children [Articles:21054454, 23719833]. APAP can be synthesized in the body through O-dealkylation of the prodrug phenacetin, a pain-killer that was withdrawn from the market due to nephrotoxicity and carcinogenesis [Article:7002186]. At the therapeutic adult dose of 1-2 g/day, oral APAP is indicated for fever and mild to moderate acute pain conditions [Article:23719833]. Administration of acetaminophen via intravenous route has become increasingly widespread and has been used as a safe and effective antipyretic and analgesic agent [Article:25521845]. Maximum recommended therapeutic dose of APAP is 4 g/day in adults and 50-75 mg/kg/day in children. Consumption of a single dose greater than 7 g in an adult and 150 mg/kg in a child is considered potentially toxic to the liver and kidneys due to the highly active metabolite N-acetyl-p-benzoquinone imine (NAPQI)[Article:22998987].
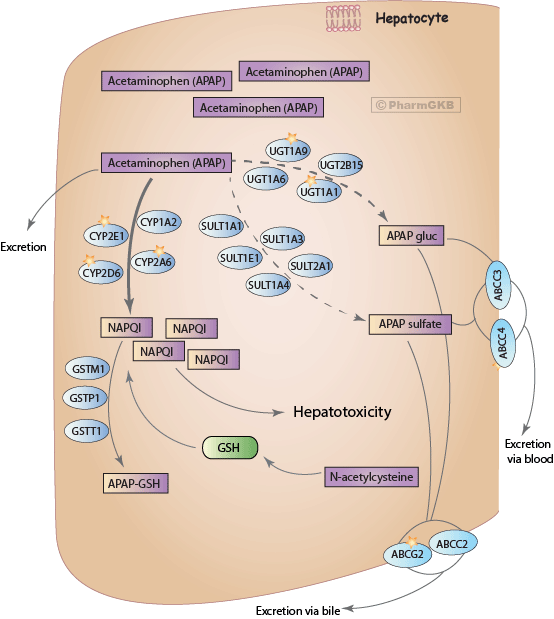
The liver, and to a lesser extent the kidney and intestine, are the major organs implicated in the metabolism of acetaminophen [Article:11215692]. After a therapeutic dose, APAP is mostly converted to pharmacologically inactive glucuronide (APAP-gluc, 52-57% of urinary metabolites) and sulfate (APAP sulfate, 30-44%) conjugates, with a minor fraction being oxidized to a reactive metabolite NAPQI (5-10%) (/pathway/PA165986279). Less than 5% of APAP is excreted unchanged [Article:6343056]. NAPQI is highly reactive and is primarily responsible for acetaminophen-induced hepatotoxicity. Detoxification of NAPQI occurs through its binding to the sulfhydryl group of glutathione (GSH) to form APAP-GSH, which is ultimately excreted in the urine as cysteine and mercapturic acid conjugates (APAP-cys) [Articles:22998987, 11215692]. Acetaminophen disposition involves a complex interorgan transport of metabolites between the liver, kidney and intestine, through bile and blood stream, to be ultimately eliminated in urine and feces [Article:11215692]. From the liver, most of glucuronide and sulfate metabolites get transported into the kidneys through the blood stream, while some APAP-gluc appears in the bile with subsequent transport into the intestine. The kidney is the main site of the disposition of APAP sulfate, either through direct excretion or through further biotransformation followed by renal excretion. Although most of NAPQI is formed in the liver, the kidney also metabolizes APAP to the toxic metabolite and releases cysteine conjugate of APAP into the bile and blood for further elimination in urine [Article:11215692].
At supratherapeutic doses of APAP (more than 4 g/day), sulfation pathway becomes saturated, while glucuronidation and oxidation increase, and a smaller amount is excreted unchanged. After a highly toxic dose of APAP, glucuronidation gets saturated as well and higher proportions of the drug are eliminated unchanged (~10%) and get oxidized to NAPQI (>15%). Excess NAPQI eventually depletes GSH stores and starts to form protein adducts through binding to cysteine groups on cellular proteins. NAPQI primarily targets mitochondrial proteins and ion channels leading to the loss of energy production, ion misbalance and cell death [Articles:22998987, 11215692, 14625346]. Following animal studies, N-acetylcysteine (NAC) was shown to be an effective antidote for acetaminophen overdose in humans [Article:7469630]. NAC replenishes GSH stores, scavenges reactive oxygen species in mitochondria and enhances the sulfation metabolic pathway. If administered within 8-10 hours after an acute overdose, NAC reduces the risk of hepatotoxicity to less than 5%. Overall, NAC prevents liver damage, renal failure and death, and is the treatment of choice for APAP poisoning [Articles:22998987, 11215692, 6343056, 3059186]. Extremely high doses of APAP result in severe liver damage accompanied by dramatically diminished glucuronidation and sulfation capacities [Article:6343056]. In patients with fatal centrilobular hepatic necrosis, plasma and urinary levels of glucorinide metabolite are almost undetectable [Article:4788034].
Glucuronidation pathway of acetaminophen metabolism is catalyzed by UDP-glucuronosyl transferases (UGT). UGTs make APAP molecule more water-soluble by transferring the glucuronosyl group from UDP-glucuronic acid [Articles:22998987, 23462933]. Studies in human liver microsomes and cultured hepatocytes indicate that UGT1A1, UGT1A6, UGT1A9 and UGT2B15 are involved in APAP glucuronidation [Articles:8494539, 11714888, 16696573, 15933229]. UGT1A6 is important at low APAP concentrations [Article:11714888], while UGT1A9 and UGT1A1 contribute the most at toxic doses with UGT1A9 catalyzing within a broad range of pharmacologically relevant APAP concentrations [Articles:11714888, 16696573].
A family of cytosolic enzymes, called sulfotransferases (SULT), carries out sulfation of acetaminophen. SULTs transfer a sulfo group from a substrate PAPS to APAP making it more polar and prone to elimination [Article:23462933]. Using human platelet homogenates as a model for xenobiotic metabolism in the liver, SULT1A1 and SULT1A3/4 were first shown to catalyze APAP sulfation [Article:6950087]. Human SULT1A3 and SULT1A4 genes are very closely related and code for identical SULT proteins [Article:14676822]. In addition to SULT1A1 and 1A3/4, sulfation of APAP in the human fetal liver is carried out by SULT1E1 and SULT2A1 [Article:18232020]. This study showed that in the fetal liver, SULT1A3/4 plays the major role in APAP sulfation; in the postnatal development, however, APAP is predominantly sulfated by SULT1A1 and SULT2A1, while SULT1A3/4 activity diminishes [Article:18232020].
Cytochrome P450 enzymes catalyze oxidation of acetaminophen to the reactive metabolite NAPQI [Articles:23462933, 11215692]. The exact contribution of particular CYP isoforms to APAP bioactivation varies and depends on the concentration of the drug. In human liver microsomes, CYP2E1 and CYP1A2 were first reported to convert high doses of APAP to NAPQI [Article:2729995]. Later studies with purified human proteins or human liver microsomes and specific inhibitors confirm the role of CYP2E1 in bioactivation of toxic levels of APAP but also report involvement of CYP2A6 [Articles:9548799, 11866476]. Studies with healthy human volunteers pre-treated with CYP2E1 inhibitor disulfiram further confirm the role of CYP2E1 in APAP oxidation [Article:10741631]. Using human liver microsomes and human recombinant CYP2D6, this enzyme has been reported to oxidize only very high, toxic doses of APAP, when plasma APAP concentration reaches 2 mM [Articles:11095574, 19219744]. The role of CYP3A4 in APAP metabolism is controversial, with findings ranging from no significant contribution to the primary role in APAP oxidation [Articles:10741631, 19219744, 8387297, 8374050].
Conjugation of NAPQI to GSH occurs via both a spontaneous process and an enzymatic reaction catalyzed by glutathione-S-transferases (GSTs) [Article:3395122]. Nonenzymatic reaction yields a GSH conjugate, 3-(glutathione-S-yl)-acetaminophen (APAP-GSH); a reduction product, free APAP; and an oxidation product, glutathione disulfide (GSSG). GST reaction yields APAP-GSH and free APAP. The human cytosolic GST family is comprised of seven distinct classes of enzymes with numerous genetic variants within each class [Article:23201197]. Human in vitro studies with isolated liver and placenta GSTs have shown that GSTP1 is the most effective catalyst of NAPQI conjugation with GSH, followed by GSTT1 and GSTM1 [Article:3395122]. In the NAPQI reduction reaction, the most efficient human transferase is GSTT1, followed by GSTM1 and GSTP1.