About this pathway
Paroxetine is a selective serotonin reuptake inhibitor (SSRI) used for the treatment of depression, panic, anxiety, obsessive compulsive disorders (OCD) and other related disorders. The SSRIs fluoxetine, fluvoxamine, paroxetine, sertraline, and citalopram vary in their pharmacological profile resulting in differential efficacy and side-effect profile for particular patients [Articles:10674711, 20393946]. SSRIs have a high affinity for serotonin transporter (SLC6A4), low affinity for noradrenaline uptake transporter, and very low affinity for neurotransmitter receptors. Paroxetine has the strongest inhibition of serotonin uptake but is less specific than other SSRIs when compared to inhibition of norepinephrine uptake (reviewed in [Article:10674711]). Based on in vitro inhibitory data paroxetine has the strongest inhibition of serotonin uptake but is less specific than other SSRIs when compared to inhibition of norepinephrine uptake (reviewed in [Article:10674711]). In vivo data suggest that escitalopram is superior in producing higher extracellular serotonin levels, presumably trough an additional interaction with the allosteric site of the SLC6A4 [Article:24424469].
Pharmacokinetics
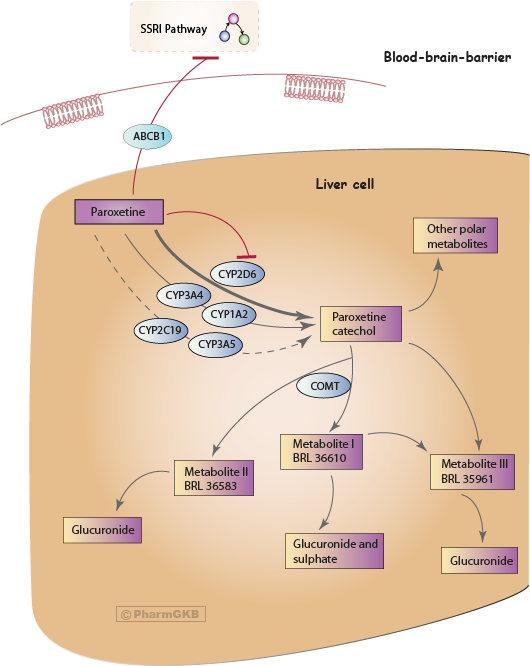
Paroxetine is well absorbed from the gastrointestinal tract and undergoes first pass metabolism in the liver. The parent drug is converted to inactive metabolites. The main enzyme involved in the transformation of paroxetine to the paroxetine catechol intermediate is cytochrome P450 2D6 (CYP2D6) (see Figure) [Articles:1388041, 1531951, 2530793]. The kinetics of paroxetine elimination is best described by a high-affinity saturable process which studies correlated with CYP2D6 activity and an additional low-affinity linear process [Articles:1388041, 1531951, 2530793].
In-vitro experiments imply a minor involvement of CYP1A2, CYP3A4/5, and CYP2C19 in the paroxetine catechol formation [Article:20007670]. The study ranks the involvement in the formation as CYP2D6 >> CYP3A4 > CYP1A2 > CYP2C19 > CYP3A5. A population-based simulation calculated that CYP3A4 and CYP1A2 are most likely to be involved in paroxetine metabolism in individuals with impaired CYP2D6 activity (CYP2D6 poor metabolizers (PM)) [Article:20007670].
Paroxetine catechol is eliminated as conjugates of subsequent metabolites M-I (BRL 36610; (3S,4R)-4-(4-fluorophenyl)-3-(4-hydroxy-3-methoxyphenoxymethyl)piperidine), M-II (BRL 36583; (3S,4R)-4-(4-fluorophenyl)-3-(3-hydroxy-4-methoxyphenoxymethyl)piperidine), M-III (BRL 35961; (3S,4R)-4-(4-fluorophenyl)-3-(hydroxymethyl)piperidine) and other polar metabolites [Articles:2530793, 10595721, 1531950, 12818234]. It is methylated by catechol-O-methyltransferase (COMT) to metabolites M-I and M-II (Figure1) [Articles:10755376, 1531950]. The enzymes involved in the creation of the glucuronide and sulfate conjugates are to our knowledge not reported so far.
Unmetabolized paroxetine is excreted to less than 2% in the urine [Article:2530793]. Its metabolites are excreted both in urine and feces [Article:2530793]. Steady state plasma concentrations were reached within 7-14 days using daily doses of 20-30mg paroxetine [Articles:2530793, 18983224].
Paroxetine is a strong CYP2D6 inhibitor, which might influence its own metabolism leading to phenocopy of metabolizer (geno-) types after continuous administration, as well as CYP2D6-dependent co-administrated drug. Studies show an effect on metoprolol [Article:21923449], clozapine [Article:11147928], desipramine [Articles:8513845, 9241008], imipramine [Article:8930024] and a combination of dextromethorphan and quinidine [Article:22283559] plasma concentrations and on its own metabolism [Article:15570195].
Patients treated with paroxetine are vulnerable to SSRI discontinuation syndrome at treatment termination [Articles:9646889, 10827885]. The shorter half-life time of paroxetine compared to other SSRIs is suggested as risk factor for these events [Article:9646889]. No differences between patient groups with and without paroxetine discontinuation syndrome are apparent in CYP2D6 poor (PMs), intermediate (IMs) or extensive metabolizers (EMs) [Article:20075642]. Ultrarapid metabolizers (UMs) have not been studied in association with paroxetine discontinuation syndrome at this point, but given that drug half-life might be shorter in UMs due to more rapid metabolism, the effect might be more pronounced in these patients.
The establishment for a clear relationship between SSRI (paroxetine) dose and plasma concentration and clinical response seems challenging [Article:10774624]. Paroxetine inhibits its own metabolism via inhibition of CYP2D6 which results in a nonlinear kinetics (Figure 1). Therefore it may be more challenging to predict plasma concentrations based on dose since higher paroxetine doses lead to a disproportionate increase in plasma concentrations.
Depressed patients are often treated with 10-40 mg/day paroxetine [Articles:18641553, 14639062, 15349705, 14514498], the dose might be higher for patients suffering from OCD [Article:20174590]. For paroxetine, it seems that lower levels of paroxetine seem most beneficial, when plasma level-response relationship is assessed [Articles:15902581, 21537937]. Although this is not consistently found [Article:17395353].
Hiemke et al. established a therapeutic reference range of 30-120 ng/ml for paroxetine, however the recommendation for therapeutic drug monitoring (TDM) is only established as 'useful', as plasma concentrations related to the pharmacodynamics effects are not yet available or based on retrospective analysis of TDM data [Article:22053351].
Pharmacogenomics
Pharmacokinetic genes
CYP2D6 is highly polymorphic and its influence in the wide interindividual variability of metabolism of a multiple drugs is well established. Pharmacokinetic parameters at steady state are dependent on CYP2D6 genotype/activity and are different among those with 0, 1, 2, or >2 active CYP2D6 alleles [Articles:10824636, 16319918, 16669849, 15349705, 17256449, 20174590].
A number of studies investigated the influence of CYP2D6 variation on paroxetine pharmacokinetic parameters, clinical outcome and frequency of side effects. A summary of studies reporting pharmacogenetics finding for CYP2D6 and paroxetine is available on ClinPGx, see Clinical Annotation.
Major findings can be summarized by considering different CYP2D6 metabolizer phenotypes. Low or undetectable paroxetine serum or plasma concentrations are reported in UMs who have high CYP2D6 activity levels (genotyped as CYP2D6*1/*2xN, *1/*1xN or *2/*2xN) [Articles:18641553, 16633156, 14639062, 12173784]. Two studies, two case reports and a study with four CYP2D6*1/*xN patients, suggest that patients with more than two active CYP2D6 alleles may have an increased risk for non-response to paroxetine treatment [Articles:18641553, 16633156]. This is further substantiated by multi-antidepressant drug studies. The frequency of UM patients treated with antidepressants metabolized by CYP2D6 is higher in the non-response group as compared to patients with non-UM phenotypes or UM frequency in general population [Articles:15116051, 14652703]. In patients with OCD carrying either no functional alleles or more than two functional alleles have a higher number of failed antidepressants medication trials compared to CYP2D6 EMs [Article:23545896].
The Pharmacogenetics Working Group of the Royal Dutch Pharmacists Association in 2011 recommends to use an alternative SSRI such citalopram or sertraline in patients with the UM phenotype [Article:21412232]. Others extrapolate dose adjustments from differences in oral clearance at multiple dose conditions from the available studies, and recommend an increase in paroxetine dose for UMs [Article:22565785]. The Clinical Pharmacogenomics Implementation Consortium (CPIC) has published a guideline for CYP2D6 and paroxetine [Article:25974703]. The guideline recommends to chose an alternative drug not predominantly metabolized by CYP2D6 for CYP2D6 UM and PM subjects.
CYP2D6 inhibits paroxetine metabolism at prolonged paroxetine exposure, especially at higher doses, and can therefore change the metabolizer phenotype of an individual who has been defined by their genotype. A number of studies show that phenotypic CYP2D6 EMs have a decrease in CYP2D6 activity after prolonged paroxetine treatment and some may convert to "slow EMs" or phenotypic PMs especially at higher paroxetine doses [Articles:12173784, 1531950, 12352271, 12870705, 17256449, 9429230, 23437966, 8880055, 10211917]. Results from Lam et al. show that while some CYP2D6 EMs may phenocopy, an incidental finding for an UM could not show an effect of paroxetine inhibition on the CYP2D6 activity [Article:12173784]. On the other hand, four UM subjects treated with nortriptyline converted to EMs or PMs during co-treatment with paroxetine 40 mg/day [Article:11673748].
Significant differences in pharmacokinetic parameters have been documented between CYP2D6 EMs and PMs (genotyped or phenotyped). At a single dose, decreased clearance of paroxetine and an increased median area under the curve (AUC) are shown [Articles:10434486, 1531950]. Similarly a significant decrease in paroxetine plasma concentrations [Articles:14639062, 1531950], increased median AUC, plasma half-life and decreased clearance [Article:1531950] are found at steady-state treatment conditions for CYP2D6 PM compared to EM. Sindrup et al. shows that the differences are much more pronounced at single dose but reduce significantly during longer treatment supporting the inhibitory effect of paroxetine on CYP2D6 [Article:1531950]. Also plasma concentrations at steady-state are increased for individuals carrying one non-functional allele vs. two functional alleles but the differences are not significant [Articles:18641553, 20174590, 10505591, 17256449].
Although a clear association of CYP2D6 variations with the pharmacokinetics of paroxetine exits between EM and PMs, this has not consistently been translated to an effect on response or risk of side effects. Several observational reports of adverse effects that also led to discontinuation are published for individuals carrying one or two non-functional alleles or reduced functional alleles, however also for carriers of two functional alleles [Articles:15544025, 12057035, 11401659, 11910262, 16319918]. Patients phenotyped as PMs experienced significantly more sexual dysfunction as a paroxetine treatment side effect compared to phenotypic EMs [Articles:17541852, 12870705] but no association for common side effects was found [Article:12870705]. On the other hand, no significant differences could be established for paroxetine-induced adverse effects (hyponatremia, nausea, severity of adverse events or the frequency of discontinuation) in PMs/IMs vs. EMs [Articles:14514498, 12404686, 16534507]. The treatment outcome is also not related to CYP2D6 genotype/phenotype [Articles:14514498, 17541852, 18641553, 20174590].
Studies investigating multiple antidepressants show that CYP2D6 PMs have an increased risk for adverse effects, a shorter time between first drug administration and dose reduction or termination of therapy [Article:15116051]. Also patients not carrying a CYP2D6 EM phenotype have a higher number of failed antidepressants medication trials than CYP2D6 EMs [Article:23545896].
Since the results are less clear for subjects carrying the CYP2D6 PM phenotype, the Pharmacogenetics Working Group of the Royal Dutch Pharmacists Association published no therapeutic dose recommendations for paroxetine in patients with the PM phenotype [Article:21412232]. Stingl et al. 2013 reports a 51% clearance in PMs compared to 100% assumed for EMs from a metaanalysis of the available pharmacokinetic studies which would suggest a decrease in paroxetine dose for PMs [Article:22565785].
As mentioned above, other CYP-450 genes might be involved to a minor extent in the paroxetine inactivation process [Article:20007670]. An article exists linking variants in the CYP1A2 gene to paroxetine treatment response but CYP2D6 variations were not studied at the same time [Article:21121774].
Pharmacodynamic genes
In addition to variations in pharmacokinetic genes, polymorphisms in pharmacodynamic genes have been studied in association with paroxetine treatment response and side effects.
The exact antidepressant mechanism of SSRIs is not understood yet. But SLC6A4 is a target for paroxetine and other SSRIs inhibiting the reuptake of serotonin in from the synaptic cleft leaving more serotonin available for neurotransmission through serotonin receptors (HTRs) (see the SSRI Pathway, PD [Articles:9400006, 7969065].
An indel polymorphism in the promoter region of SLC6A4 is intensively studied and mostly reported as a long (L) version and a short (S) version with a length difference of 44 bp [Articles:8632190, 8788073, 16402131, 9605856, 10673766]. Additional long and short alleles of different sequences/lengths are identified [Articles:9605856, 10673766]. The short allele of the indel polymorphism is associated with lower gene expression [Articles:8632190, 8929413].
The polymorphism has been studied in terms of disease risk, but the studies are not conclusive and contradictory. To address this inconsistency, several meta-analyses have been carried out; linking the SS genotype as a risk factor for post-traumatic stress disorder in high trauma exposure [Article:24222274], establishing no relationship between the indel polymorphism and borderline personality disorder [Article:23810197] or panic disorder [Article:17705872]. For depression a meta-analysis is underway [Article:24219410].
The polymorphism has been also investigated in pharmacogenetic studies. Asian population studies report an improved treatment response to paroxetine for SS allele carriers ([Articles:21688171, 19259652]-Panic disorder, [Article:10683861]-Depression), while others report an association with the L allele ([Article:16874005]-Anxiety, [Article:15812265]-Depression) and further studies found no conclusive association for this polymorphism with response to paroxetine ([Articles:19606452, 16874005]-Depression). Conversely, in Caucasian populations, the LL genotype is associated with increased response ([Articles:17853254, 17914325]-Depression) but reports showing no association also exist ([Article:19800133]-panic disorder, [Articles:15520364, 18987562]-Depression). Further no differences for paroxetine-induced nausea has been found in Asians [Article:17697394] and an increased risk of discontinuation due to adverse events in S allele carriers was found in a predominantly Caucasian cohort [Article:15520364].
Additional variants are found in the SLC6A4 promoter region, such as rs25531, which alters the functional effect of the long allele. Studies group the short allele with the long allele containing the G allele of the rs25531 variation since both seem functional equivalent and compare these to the long allele containing the A allele of rs25531.
Murphy et al. reviews the challenges of the indel association studies [Article:23336058]. Additionally, the allele frequency varies between populations; Caucasians have about 22% S/L rs25531G alleles, while Asians have about 60% [Article:23336058].
Summaries of the studies investigating this SLC6A4 indel promoter polymorphism with paroxetine treatment response and side effects are available (SLC6A4 HTTLPR long form or L allele and SLC6A4 HTTLPR short form or S allele). However, few studies for paroxetine include the rs25531 genotype to consider the triallelic effect.
Several articles are in favor of combining variants in CYP2D6, CYP2C19, CYP2C9, CYP1A2, SLC6A4, 5-hydroxytryptamine (serotonin) receptor 2A (HTR2A), and HTR2C (in one article), to guide treatment with antidepressant (including paroxetine) and antipsychotic drugs [Articles:24151799, 24229738, 23511609, 24018722, 23047243].
HTR2A and HTR2C belong to the serotonin receptor family. Variants in the HTR2C gene are mostly relevant for antipsychotic drugs in association with treatment related weight gain [Article:24151799]. HTR2A variations have been investigated for effect in drug response and side effects. The GG and GA genotypes of rs6314 are associated with better drug response compared to subjects carrying the AA genotype [Articles:18253134, 11311507]. Carriers of the GG genotype of rs6313 might experience an increased risk for side effects [Articles:18253134, 14514498], however, this result is not consistently found [Articles:17697394, 20075642], and no association with treatment response is reported [Article:19361869]. The C allele of rs6311 shows no association with treatment response [Article:16874005].
Further variations in the following serotonin-related genes or in other neurologically relevant receptors have been studied with regards to paroxetine treatment response and side effect profile: DRD3, HTR1A, HTR1B, FKBP5, and BDNF.
Transporter genes
Additionally, paroxetine is an ABCB1 substrate and is actively transported from the brain. Several variants in the ABCB1 gene are studied in association with therapeutic response to paroxetine, but the variants associated with effect vary within studies and the findings are contradictory. Uhr et al. groups antidepressants (venlafaxine, paroxetine, amitriptyline, citalopram) that are ABCB1 substrates and compares with non-ABCB1 substrate antidepressants [Article:18215618]. Using this approach, Caucasian carriers of the rs2232583 TT genotype seem to have a higher risk of being non-remitters for ABCB1 substrate antidepressants. During paroxetine treatment in a predominantly Caucasian cohort, carriers of the rs2032583 C allele went into remission faster than those with the TT genotype, but this association was not significant after Bonferroni correction [Article:20555295]. Carriers of the ABCB1 haplotype rs1045642 C (3435C>T)- rs2032582 G (2677G>T/A)- rs1128503 T (1236T>C) are associated with poorer response to paroxetine treatment based on HAM-D score change at week 6 in Japanese patients [Article:17913323]. While other studies (Caucasian cohorts) cannot confirm an association of either rs1045642 or rs2032582 with paroxetine response defined as subjects with a decrease in Hamilton Depressive Rating (HAMD) scale by >or=50% or 50% improvement from baseline Montgomery-Åsberg Depression Rating Scale (MADRS) score [Articles:18550244, 18641553, 20555295].
Conclusion
Paroxetine is substrate and inhibitor of CYP2D6. Its metabolism is affected by variation in this gene.
Subjects with more than two active CYP2D6 alleles (UM) may benefit from an alternative SSRI since paroxetine clearance is more than 150% elevated, and therefore treatment with standard doses may lead to low or undetectable plasma levels.
A clear drug plasma concentration/effect relationship does not exist for paroxetine. Additionally, during prolonged treatment especially with higher dose paroxetine's inhibitory effect leads to phenocopying, transforming a subset of EMs into IMs or PMs.
Further studies are needed to identify reliable biomarkers for SSRI treatment and investigate the effect of combining variations in pharmacokinetic and pharmacodynamic genes to guide paroxetine therapy.
Edit history (2)
- 2022-09-12 Update Fixed broken links for clinical annotations with CYP2D6 and paroxetine and to the SLC6A4 HTTLPR long form (L allele) and SLC6A4 HTTLPR short form (S allele)
- 2025-06-16 Update fixed typo