About this pathway
Background
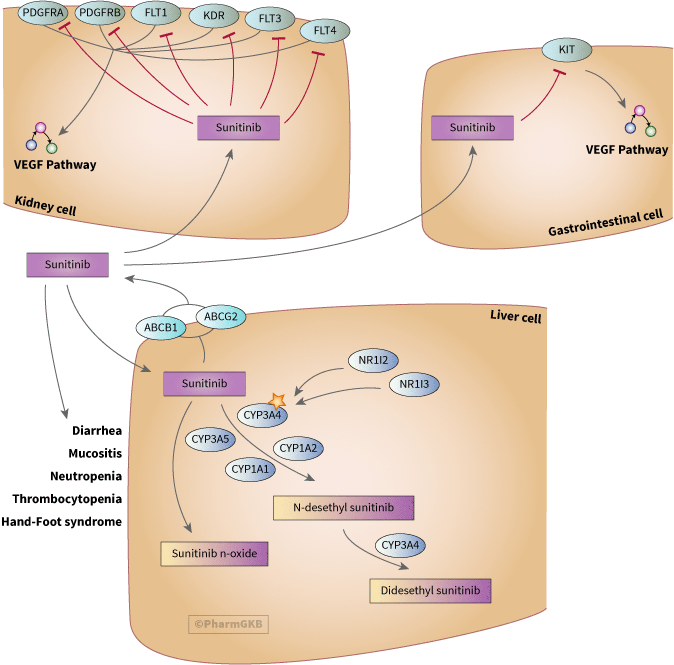
Sunitinib is a second-generation small molecule tyrosine kinase inhibitor (TKI). It is an oral multi-kinase drug inhibiting VEGF receptors (coded for by FLT1, KDR and FLT4), PDGFRs (coded by PDGFRA and PDGFRB), KIT, FLT3 and RET [Article:12538485]. Sunitinib was approved by the US FDA as a first-line of treatment of metastatic renal cell carcinoma (mRCC) and imatinib-resistant or imatinib-intolerant gastrointestinal stromal tumors (GIST) [Article:17825686].
Pharmacokinetics
Elimination of sunitinib is primarily via feces (61%) and less than 16% is excreted in urine [Article:19258444]. Most common toxicities associated with sunitinib are diarrhea, thrombocytopenia, leukopenia, mucosal inflammation and hand-foot syndrome [Articles:18594533, 17046465, 16314617, 18594533, 16757724]. Less common toxicities are cardiotoxicity and hypothyroidism [Articles:17202116, 18838713]. Sunitinib-induced hypertension may be a marker of treatment efficacy in patients with RCC. Studies indicate increased hypertension was also associated with improved time to disease progression and over all survival [Article:21208033].
Sunitinib metabolized by CYP3A4 to an active N-desethyl metabolite (SU12662), which is further metabolized to inactive metabolites [Article:17825686]. SU12662 has longer half-life, similar inhibitory profile and similar plasma protein binding to that of sunitinib. The combination of sunitinib and SU12662 represents the total active drug in plasma.
Pharmacodynamics
Clear cell RCC is characterized by inactivation of VHL causing elevated protein levels of HIF1a, which in turn upregulates VEGF and PDGF expression. Sunitinib inhibits receptor tyrosine kinases like VEGFRs and PDGFRs that interact with VEGF and PDGF respectively. These ligands play an important role in tumor angiogenesis and proliferation. Thus, sunitinib-mediated multi-targeted inhibition leads to decreased tumor vascularization and cancer cell death. Sunitinib mediates similar effects by inhibiting KIT, the RTK that drives majority of GIST tumors [Article:19248971].
Pharmacogenomics
Polymorphisms in a number of genes involved in sunitinib-mediated pharmacokinetic (NR1/2, NR1/3, CYP3A5, CYP1A1, CYP1A2, ABCG2 and ABCB1) and pharmacodynamic pathways (PDGFRa, VEGFR2, VEGFR3, RET, FLT3) affect sunitinib exposure and efficacy. Some of the SNPs associated with sunitinib outcome show large interethnic differences in allele frequency. For example, VEGFR3 rs307826 is absent or at very low frequency in Asians and Africans. Minor allele frequencies of ABCG2 rs2231142 are approximately 3 fold higher in Asians than in Caucasians [Article:19111841].
In a prospective study of 89 patients with clear cell RCC (ccRCC), presence of CYP3A5*1 (rs776746 G>A) allele was significantly associated with a higher risk of dose reductions due to dose toxicity by multivariate analysis [Article:22015057]. This association was also reported in a larger cohort of 333 patients [Article:25930089]. CYP3A5*1 is a high-activity allele, potentially increasing metabolism of sunitinib to a longer acting metabolite, SU12662, thereby increasing the risk of adverse events. Interestingly, increased levels of SU12662 may also be beneficial by increasing the efficacy of sunitinib. Presence of A allele in rs776746 was associated with improved progression-free and overall survival in a study of 136 patients with metastatic ccRCC [Article:21097692]. Presence of G allele in CYP1A1 variant rs1048943 was associated with a 4-fold increase in risk of mucosal inflammation and ~6-fold increase in risk of leukopenia during first sunitinib treatment cycle of 29 patients diagnosed with RCC or GIST [Article:19667267].
Sunitinib also has affinity for efflux transporters like ABCB1 and ABCG2 [Articles:20348146, 19773380, 18971320]. In the first prospective pharmacogenomics study of 101 patients with RCC treated with sunitinib, rs1128503 (G412G) and rs2032582 (A893S) variants of ABCB1 were associated with decreased risk for hypertension. Presence of TT genotype in rs1128503 and TT/TA genotype in rs2032582 was also associated with an increased likelihood for time to dose reduction (TTDR) [Article:24874929]. Hence, patients with these genotypes are less likely to require dose reductions compared to those with wildtype or heterozygous variants of these SNPs. Absence of TTT genotype in ABCB1 haplotype consisting of 3435C/T (rs1045642), 1236C/T (rs1128503) and 2677G/T (rs2032582) was associated with 2.6 fold reduction in risk of hand-foot syndrome [Article:19667267]. In terms of sunitinib efficacy, presence of TCG in the ABCB1 haplotype was associated with improved progression-free and overall survival [Articles:21097692, 25930089]. Although the ABCB1 haplotype is a silent mutation, it alters the function of the efflux transporter including its substrate specificity [Article:17185560]. On the contrary, presence of TT genotype in rs1128503 was associated with reduced progression-free and overall survival in another study [Article:23462807]. The above data indicate that the three ABCB1 SNPs increase ABCB1-mediated efflux of sunitinib, consequently decreasing sunitinib exposure and increasing its clearance. This in turn reduces the likelihood of adverse events like hypertension. Further, absence of TCG haplotype or presence of TT genotype in ABCB1 variants decrease sunitinib efficacy.
Genetic variations in another efflux transporter, ABCG2, also influence sunitinib-induced toxicity and efficacy. Presence of one or two copies of TT in ABCG2 haplotype consisting of -15622C/T and 1143C/T (rs2622604) increased the likelihood for higher-grade toxicity (>2) by 2.6 fold in patients with RCC or GIST [Article:19667267]. In case studies of Asian patients with mRCC, presence of AA genotype in rs2231142 variant in ABCG2 was associated with high exposure to sunitinib, most likely as result of reduced ABCG2 protein expression and activity [Articles:25515134, 19111841, 12479221, 20348146].
Polymorphisms in nuclear receptors like NR1I3 also affect sunitinib exposure. NR1I3 encodes a constitutive nuclear androstane receptor that plays an important role in regulating genes like CYP3A4, thereby involved in drug detoxification mechanism. Absence of CAT and CAG genotypes in NR1I3 haplotype consisting of 5719C/T (rs2307424), 7738A/C (rs2307418) and 7837T/G (rs4073054) was associated with 2.6 fold reduction in risk of hand-foot syndrome and 1.7 fold increase in risk of leukopenia [Article:19667267]. Presence of TT genotype in NR1I3 rs4073054 and NR1I2 rs2276707 was associated with reduced sunitinib efficacy as reflected by decreased progression and overall survival rates [Article:23462807].
Polymorphisms in gene involved in sunitinib-associated pharmacokinetic pathway have also been reported to affect sunitinib response and tolerability. Presence of VEGFR2/KDR variants rs2305948 and rs1870377 increases the likelihood of higher-grade toxicity (>2) and hypertension respectively [Articles:19667267, 22015057]. Genetic variations in VEGFR1/FLT1 and VEGFR3/FLT4, other members of VEGFR family inhibited by sunitinib, affect sunitinib efficacy. For example, presence of VEGFR3-T494A (rs307826) and VEGFR3-R1324L (rs307821) variants were associated with reduced progression-free and overall survival in patients with mRCC [Articles:22015057, 23462807]. In contrast, patients with CC genotype in VEGFR1 SNP rs9582036, AA genotype in VEGFR1 SNP rs9554320 and CC genotype in VEGFR3 SNP rs6877011 were more likely to have poorer response, progression-free and overall survival rates when treated with sunitinib [Articles:23421954, 23511629]. Different polymorphisms in VEGFR ligand like VEGFA have different implication on sunitinib exposure. Presence of TT genotype in rs833061 and CC genotype in rs699947 and rs2010963 were associated with reduced progression-free and overall survival in patients with mRCC [Article:23511629]. rs2010963 was also reported to increase the risk of sunitinib-induced hypertension [Article:21882181].
Other pro-angiogenic factors like PDGFRa and FLT3 have also been implicated in sunitinib response. Presence of GCGT haplotype composed of PDGFRA variants rs1800810, rs1800812, rs1800813 and rs35597368 in both alleles was significantly associated with reduced overall survival compared to GCG-other or other-other haplotypes in patients with ccRCC [Article:21097692]. Presence of FLT3 738C variant (rs1933437) was associated with 2.8 fold reduction in risk of leukopenia and thrombocytopenia in patients with RCC or GIST after one cycle of sunitinib treatment [Articles:19667267, 20683446].
Reactions & interactions (36)
-
Activation
NR1I3 → CYP3A4
-
Activation
NR1I2 → CYP3A4
-
Biochemical Reaction
n-desethyl sunitinib → n,n-didesethyl sunitinib
-
Biochemical Reaction
sunitinib → n-desethyl sunitinib
-
Biochemical Reaction
sunitinib → sunitinib n-oxide
-
Catalysis
CYP3A4 → Biochemical Reaction
-
Catalysis
CYP3A4 → Biochemical Reaction
-
Catalysis
CYP1A2 → Biochemical Reaction
-
Catalysis
CYP3A5 → Biochemical Reaction
-
Catalysis
CYP1A1 → Biochemical Reaction
-
Catalysis
ABCB1 → Transport
-
Catalysis
ABCG2 → Transport
-
Inhibition
sunitinib → ABCB1
-
Inhibition
sunitinib → ABCG2
-
Inhibition
sunitinib → FLT4
-
Inhibition
sunitinib → KIT
-
Inhibition
sunitinib → KDR
-
Inhibition
sunitinib → FLT1
-
Inhibition
sunitinib → FLT3
-
Inhibition
sunitinib → PDGFRB
-
Inhibition
sunitinib → PDGFRA
-
Leads To
PDGFRB → VEGF Signaling Pathway
-
Leads To
sunitinib → mucositis
-
Leads To
PDGFRA → VEGF Signaling Pathway
-
Leads To
KIT → VEGF Signaling Pathway
-
Leads To
sunitinib → Diarrhea
-
Leads To
sunitinib → Neutropenia
-
Leads To
sunitinib → Thrombocytopenia
-
Leads To
sunitinib → hand-foot syndrome
-
Leads To
FLT3 → VEGF Signaling Pathway
-
Leads To
KDR → VEGF Signaling Pathway
-
Leads To
FLT4 → VEGF Signaling Pathway
-
Leads To
FLT1 → VEGF Signaling Pathway
-
Transport
sunitinib → sunitinib
-
Transport
sunitinib → sunitinib
-
Transport
sunitinib → sunitinib
Edit history (2)
- 2018-04-09 Create
- 2019-02-25 Update Updated to new illustrator formatting.