About this pathway
Background:
Gemtuzumab ozogamicin (GO) is an immunoconjugate between an anti-CD33 antibody and a cytotoxic calicheamicin derivative (N-acetyl g1 calicheamicin). N-acetyl g1 calicheamicin is part of the enediyne family and causes single- and double-stranded DNA breaks followed by DNA repair or, if damage is overwhelming, apoptosis and cell death. CD33 is a 67kD glycoprotein transmembrane receptor expressed on the cell surface of myeloid lineage cells. The extracellular portion of the CD33 receptor contains IgG domain antigens that allow for antibody conjugate formation. As a myeloid differentiating antigen, CD33 is estimated to be present on malignant blast cells of approximately 85-90% of patients with acute myeloid leukemia (AML) [Article:12576328]. The observation that antibodies were internalized after binding to CD33 led to the development of GO [Articles:11342449, 15454492].
As the first cancer immunoconjugate ever to receive FDA approval, GO was indicated for the treatment of CD33+ AML in first relapse for patients greater than 60 years of age who were not considered candidates for conventional chemotherapy [Article:11410481]. This approval was based on results from interim analyses of phase 2 monotherapy trials showing achievement of complete remission (CR) or CR with incomplete platelet recovery (CRp) in approximately 30% of such patients. Unfortunately, findings of the Southwest Oncology Group (SWOG) S0106 trial showing lack of benefit of GO across the entire study population as well as slightly higher treatment related mortality (TRM) led the manufacturer of GO to withdraw commercial drug availability in the United States in 2010 [Article:23591789]. It is currently only available commercially in Japan. However, the study was limited in several ways. First, the dose of daunorubicin was only 45 mg/m2 in the GO arm compared with 60 mg/m2 in the standard arm without GO. Previous studies in AML have shown an increase in overall survival with dose intensification of anthracyclines in induction therapy. Therefore, the difference in anthracycline dose between the two arms renders them difficult to compare. In addition, the 5% rate of mortality in the study arm with GO is consistent with the majority of the studies in AML, whereas the mortality of 1% observed in the control arm without GO is remarkably lower and inconsistent with previous studies [Articles:23591788, 23591789]. Since this trial, several other studies have shown that GO is active in AML and has acceptable toxicity when used at 3-6 mg/m2 doses, few studies have shown that GO has significant survival benefits for a certain subset of patients, particularly those within the favorable risk group [Articles:23591789, 22482940, 21172891, 24006085]. In addition to AML, GO has shown effectiveness in treatment of acute promyelocytic leukemia [Articles:21142804, 19075265].
GO Pathway Description:
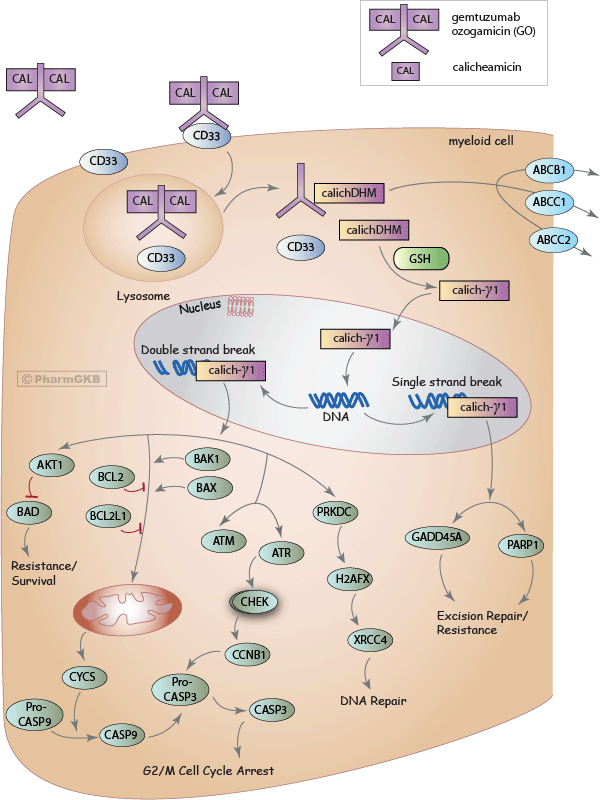
In GO, the unconjugated antibody itself is largely non-toxic and primarily facilitates uptake of the calicheamicin derivative into CD33+ cells. The CD33 antigen is expressed on both normal colony forming cells (CFC) and most of the AML cells including leukemic clonogenic precursors but not on normal pre-CFC, pluripotent hematopoietic stem cells, or non hematopoietic tissue. Approximately 90% of adult and pediatric AML patients have myeloid blasts that express CD33 thereby making this target attractive for the treatment of AML [Articles:2937468, 3470307, 10910899]. Upon binding to CD33, GO-CD33 complex is rapidly internalized. This involved phosphorylation of cytoplasmic immune-receptor tyrosine-based inhibitory motifs (ITIM) most probably by the Src Family Kinase (LCK), which then stimulates endocytosis of the GO-CD33 complex [Articles:17947393, 23747885]. The complex is translocated into lysosomes where the bifunctional acid-hydrolyzable linker between the antibody and calicheamicin is cleaved in the acidic environment, thereby releasing the calichDMH derivative [Articles:11792178, 15592433]. CalichDMH is then reduced by glutathione to form the 1,4-dihydrobenzene diradical species [Article:15592433]. This highly reactive form enters the nucleus and binds to the minor groove of the DNA, causing DNA double strand breaks and DNA single strand breaks [Articles:15592433, 12606118]. It is proposed that this DNA damage stimulates two different DNA damage response pathways.
Mitochondrial Mediated Apoptosis: Once DNA damage occurs, the mitochondrial apoptosis signaling cascade is initiated by the activation of proapoptotic proteins BAX and BAK1 [Article:19463775]. BAX and BAK1 activation results in the mitochondrial permeability transition. Cytochrome C is released, which results in processing of procaspase 9 to caspase 9. Caspase 9 activates processing of procaspase 3 to caspase 3 [Articles:15592433, 14647446], which then leads to cell death. It has also been demonstrated that there is a caspase-mediated auto-amplification loop necessary for full mitochondrial pathway activation 14647446. Studies have demonstrated that inhibition of this apoptotic pathway occurs via anti-apoptotic proteins BCL2 and BCL2L1, which are regulators of cytochrome C release. Overexpression of BCL2 and BCL2L1 inhibits GO cytotoxicity [Articles:12576328, 15592433].
Ataxia-Telangiectasia Mutated/Ataxia-Telangiectasia Related (ATM/ATR) Pathway Mediated Cell Cycle Arrest: Studies also show that the ATM/ATR pathways are activated in response to DNA damage. Once DNA double strand breaks occur, KU80 and RPA3 proteins get involved in double strand processing [Article:22632031] and ATM/ATR kinases are phosphorylated and activated [Articles:12576328, 15592433]. These subsequently phosphorylate checkpoint kinase 1 (CHEK1) and checkpoint kinase 2 (CHEK2) [Articles:12576328, 15592433]. Activated CHEK1 and CHEK2 are responsible for the up-regulation of cyclin B1, leading to cell cycle arrest through caspase 3 activation [Articles:12576328, 15592433].
Induction of DNA damage and cell death: The activated diradical calicheamicin derivative scavenges oxygen and initiates conformation dependent single or double strand DNA scission, thus primarily inducing DNA damage. In response to DNA double strand break, initiation of repair occurs via activation of DNA-dependent protein kinase (DNA-PK). Activation of DNA-PK in turn leads to activation of H2A by phosphorylating to the minor histone2A variant (H2AFX) [Article:20493860]. Multiple other proteins are involved in the process of DNA damage repair, including the x-ray repair cross-complementing group 5 (XRCC5), the x-ray repair cross-complementing group 4 (XRCC4) and Ligase 4 complex. DNA double strand breaks also activate the AKT signaling pathway which reduces the cytotoxicity induced by calicheamicin [Article:23320091]. In fact, cells with impaired DNA repair pathways have been shown to be highly sensitive to calicheamicin induced cell death [Articles:1700294, 12606118]. Calicheamicin also produces DNA single strand breaks. GADD45A and PARP1 are associated with DNA excision repair for single strand breaks [Articles:12606118, 22632031, 2109651]. Although detailed studies on understanding the precise pathway/genes in the GO mediated DNA damage repair pathway are required, inhibition of AKT increases GO sensitivity [Article:23320091].
Inhibition of Mitochondrial mediated apoptosis: Inhibition of the mitochondrial mediated apoptotic pathway occurs via anti-apoptotic proteins BCL2 and BCL2L1 which are regulators of cytochrome C release. Overexpression of BCL2 and BCL2L1 inhibits GO cytotoxicity by down-regulating mitochondrial permeability transition activation and cytochrome C release [Articles:12576328, 15592433]. Recent data in HL60 cells lines made resistant to GO and/or cyclosporin (MDR1 inhibitor), showed DNA repair proteins to be critical for efficacy of GO [Article:22632031].
Cellular parameters important for GO mediated cytotoxicity:
Multiple studies have suggested several cellular parameters that are important for GO mediated cytotoxicity as well as for development of GO resistance [Articles:15029214, 17530021]. Efficacy to GO might be modulated by factors described below.
CD33 expression: Although the majority of patients with AML express CD33 on malignant blast cells, CD33 expression levels in peripheral blood measured by flow cytometry within these patients have been shown to be heterogeneous [Article:22378848]. GO has been shown to be selectively cytotoxic to CD33+leukemia cells relative to those lacking CD33 expression [Article:11792178]. In vitro studies using cell lines expressing high levels of CD33 have revealed a quantitative relationship between CD33 expression and GO cytotoxicity, indicating that antigen density correlates with drug susceptibility in these cell lines. The rate of CD33-GO internalization directly correlates with GO cytotoxicity [Article:15454492]. As discussed previously, the CD33 ITIMs control CD33-GO endocytosis. After phosphorylation of the ITIMs, the suppressor of cytokine signaling 3 (SOCS3) protein is recruited and competes with SHP1/2 binding to the ITIMs. In the presence of SOCS3 binding to the ITIM, proteasomal degradation of CD33 is accelerated; suggesting that expression of SOCS3 may result in resistance to GO therapy [Articles:17008544, 23747885]. However recent in vivo data although suggest expression of CD33 to be very heterogeneous in AML patients, higher CD33 expression has been associated with adverse disease characteristics and hence as a predictor of poor outcome [Article:22378848].
Internalization of CD33-GO complex: Efficient binding of CD33 and GO is a critical requirement for internalization of CD33-GO complex. The ITIM domain of CD33 has been implicated in internalization of antibody bound CD33. Disruption of cytoplasmic ITIM motif of CD33 (by introducing point mutations) has been shown to prevent efficient internalization of the GO-CD33 complex. This block in internalization significantly reduced GO-induced cytotoxicity in cells expressing ITIM mutant CD33 [Article:15454492]. These results imply the importance of the quantity of GO-CD33 complex internalization for GO mediated cytotoxicity.
Calicheamicin release and activation: Lysosomal cleavage of GO releases the calicheamicin moiety, which is then reduced to a highly reactive 1,4-dehydrobenzene diradical through glutathione. The quantity of calicheamicin released upon hydrolysis and the presence of the activated form of calicheamicin in the cell therefore influences GO cytotoxicity. One of the proposed mechanisms of resistance is through efflux of calicheamicin mediated by members of the ATP-binding cassette (ABC) transporter proteins. The multidrug resistant protein MDR1 (ABCB1) influences GO chemosensitivity; further in vitro studies using modulators of MDR1 activity have been shown to alter GO sensitivity. This was supported in a study by Walter et al. in which non-responders to GO were found to have higher MDR1 activity compared to responders [Article:17227830]. In addition to ABCB1 also ABCC1 (MRP1), ABCC2 (MRP2) has been suggested in modifying GO resistance [Articles:12576328, 15592433, 12689934, 11986941, 18271955].
Metabolic fate and pharmacokinetics (PK) of GO and calicheamicin
The metabolism of GO mainly involves the activation and metabolism of the non-antibody, active component of GO, NAc-gamma calicheamicin DMH. The metabolism of GO has been investigated in human liver microsomes (HLM), human liver cytosol (HLC) and human leukemia cells (HL-60). A total of 11 metabolites were found after incubation with GO. Both HLM and HLC metabolites were found in human hepatocytes after GO therapy, suggesting that NAc-gamma calicheamicin may be transported into human hepatocytes. In vitro assays have demonstrated that several enzyme systems in HLM, HLC and hepatocytes are involved in the metabolism of calicheamicin. Oxygenation and methylation are the main biotransformation pathways involved in liver microsomes, whereas the acetylation of calicheamicin and its derivatives are the major pathways involved in cytosol. The three major enzyme systems involved are esterases, carbonyl reductase, and cytochrome P450 3A4 (CYP3A4) in the oxidative metabolism steps. While CYP3A4 is the major enzyme involved in the oxidative metabolism of NAc-gamma calicheamicin, it results in transformation into other non-oxidative metabolites; therefore inhibition of CYP3A4 is not likely to contribute to significant drug-drug interactions [Article:11410481]. A phase 2 study in adult AML patients with first relapse performed GO PK analysis by measuring the levels of GO, total and conjugated calicheamicin derivatives in plasma samples obtained at several time points [Article:11697753]. Following first dose of 9mg/m2 the peak plasma concentration of GO was 2.86 ± 1.35mg/L and half-life was 72 ± 42 hrs. The PK profiles of total and conjugated calicheamicin were observed to be similar to GO [Article:11697753].
In pediatric patients with refractory/relapse AML following 9 mg/m2 dose GO PK profile followed similar pattern to adult patients with Cmax being 3.47± 1.04mg/L and half-life being 64± 44 h after first dose [Article:15286091]. Both studies suggest wide inter-patient variation in various PK parameters (total and unconjugated calicheamicin plasma levels). No influence of gender and age was observed in the PK of GO [Article:11601662].
Pharmacogenetics
Since CD33 is the target of GO, any genetic variation in CD33 that can influence its expression, surface localization or physiological role can have an impact on patient's response to GO. In a pilot study of 22 pediatric AML patients who received GO-based therapy on the St. Jude AML02 trial, Lamba et al., sequenced the coding regions of CD33 gene and demonstrated an association between genetic polymorphism in CD33 gene and clinical response to GO [Article:18615103]. A total of 9 SNPs (7 coding, 1 intronic and 1 in 3'UTR) were identified and of 7 coding SNPs. Of these 4 non-synonymous coding SNPs and the 3'UTR SNP occurred with the minimum allele frequency of >10%. Although the sample size was small (n=22), CD33 coding SNP Ala14Val (rs12459419; C>T) was found to be associated with minimal residual disease (MRD) after GO therapy [Article:18615103].
A follow up study in a larger cohort of pediatric AML patients (COG, AAML03P1; n=242) receiving GO based therapy (GO), significant correlation of CD33 SNPs with its cell surface expression on leukemic blasts, clinical characteristics and treatment outcome [Article:23444229]. CD33 SNP Ala14Val (rs12459419; C>T) was significantly associated with lower median diagnostic blast CD33 expression (P < 0.001); additionally patients with TT genotype were more likely to have favorable risk disease as compared to patients with CC and CT genotypes, (52% vs. 31%, P = 0.034) and improved 3-year overall survival. CD33 coding SNP Arg69Gly (rs2455069) as well as the 3'UTR SNP (rs1803254) were associated with lower CD33 expression in leukemic cells.
With respect to clinical outcome, the 3-year overall survival (OS) rate from remission was 84% ± 8% for those homozygous (GG) for Arg304Gly (rs35112940) versus 68% ± 15% for the other genotypes (P = 0.018); these patients also had a lower relapse risk (P=0.025). Patients with at least one variant allele (G) with the 3'UTR SNP (rs1803254) also had a worse 3-year TRM. Analysis of these SNPs in an independent cohort of patients who did not receive GO as a chemotherapeutic agent, showed no significant association between CD33 SNPs and clinical outcome [Article:23444229].
Recently evaluation of 1931 SNPs within Affymetrix DMET Plus Gene Chip for association with response in AML patients receiving GO with fludarabine-cytarabine-idarubicin and identified significant association between SNPs in ADH1A, SLCO1B1, SLC22A12 and SULTB1 and response/toxicity [Article:22584460]. In a small cohort of AML patients (n=21) receiving GO SNPs in GSTP and NQO1 were evaluated for association with hepatic sinusoidal occlusion syndrome (SOS). Although not statistically significant, GSTP*B variant was associated with increased risk of hepatic SOS [Article:14663169].
In summary, development and approval of GO has established the precedent for effectiveness of antibody-targeted therapies in cancer. Unfortunately, GO was withdrawn from market following the results from the phase 3 study by Southwest Oncology group [Article:23591789]. However results of at least new randomized studies as well as a study from St Jude Children's research hospital strongly support efficacy of GO with acceptable toxicity thus warranting revisiting the clinical utility of GO in AML. Understanding the genetic factors that predict GO response will help identify subsets of patients with different likelihoods of response.
Edit history (2)
- 2014-01-14 Create
- 2024-08-28 Update fixed typos