About this pathway
Introduction
Voriconazole is a triazole antifungal agent active against a variety of fungi and molds, such as Candida, Aspergillus, Fusarium, Scedosporium and Cryptococcus. It is particularly recommended for pulmonary invasive aspergillosis, an infection that primarily occurs in immunocompromised patients, such as those undergoing organ transplantation or with autoimmune conditions [Articles:22141384, 21881144]. Voriconazole and other triazole antifungals work by disrupting the synthesis of a compound found in fungal cell membranes called ergosterol. Disruption of ergosterol synthesis leads to damage to the fungal cell membrane, and eventual fungal cell death or inhibition of fungal cell growth [Article:18447660]. While voriconazole is generally well-tolerated and effective, it has a narrow therapeutic window. Drug levels that are too low can diminish efficacy, while those that are too high can affect tolerability and safety [Articles:22141384, 18171251]. Serious adverse events associated with voriconazole use include hepatotoxicity and central nervous system effects; visual disturbances are also common, particularly at higher concentrations of the drug [Article:24510446]. The metabolism and clearance of voriconazole, and consequently the levels of the drug within the body, are influenced by CYP2C19 genotype. Non-genetic factors that affect voriconazole levels include patient age, gender, liver disease and concomitant medications [Article:23442261]. Drug labels for voriconazole approved by the U.S. Food and Drug Administration (FDA) and Health Canada note that individuals who are CYP2C19 poor metabolizers exhibit, on average, 4-fold higher drug exposure as compared to normal (extensive) metabolizers. However, the evidence that supports a direct association between between CYP2C19 and toxicity or efficacy is limited. This review will provide an overview of the literature on the pharmacokinetics and pharmacogenetics of voriconazole. A particular emphasis will be given to pharmacogenetics, as developments in this area may provide a way to optimize dosing.
Pharmacokinetics
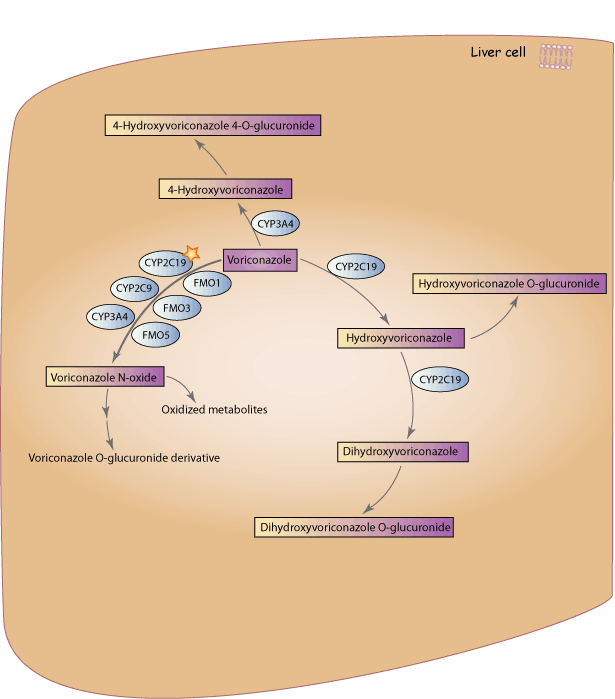
A schematic representation of voriconazole disposition within the body is provided in the figure above. Voriconazole is extensively metabolized, with less than 2% of the original dose excreted in unchanged form [Article:16802848]. The main circulating metabolite is voriconazole N-oxide, which has no antifungal activity [Articles:16802848, 12695341]. CYP2C19 is the primary enzyme responsible for the metabolism of voriconazole into voriconazole N-oxide, though CYP3A4, CYP2C9, and members of the flavin containing monooxygenase (FMO) family also contribute [Articles:16802848, 12695341, 18362161, 17433262]; it’s estimated that approximately 75% of the total voriconazole metabolism is mediated through the CYP enzymes, while the FMO family mediates the remaining 25% [Article:18362161]. Voriconazole N-oxide can also be further metabolized into various less-prevalent metabolites [Article:12756205]. Voriconazole has the potential to be both a substrate and an inhibitor of the CYP2C19, CYP3A4 and CYP2C9 enzymes [Article:16802848].
Voriconazole has two other main routes of metabolism: one is the hydroxylation of the methyl group, and the other is hydroxylation of the fluoropyrimidine ring [Articles:12756205, 18362161]. Figure 1 below shows the chemical structures for these two hydroxylated metabolites, as well as the structure for voriconazole N-oxide. The hydroxylation of the fluoropyrimidine ring is thought to occur through the action of CYP2C19, while hydroxylation of the methyl group is thought to occur through the action of CYP3A4 [Articles:18362161, 17433262, 20002085]. After hydroxylation, both metabolites form glucuronidated metabolites. Additionally, the hydroxyvoriconazole metabolite can be hydroxylated again via CYP2C19 to form dihydroxy-voriconazole; this dihydroxy metabolite can then be glucuronidated [Articles:12756205, 20002085]. Bourcier et al. found that UGT1A4 is the main enzyme involved in the glucuronidation of voriconazole, though no information about its role in glucuronidation of voriconazole metabolites is available [Article:20304965].
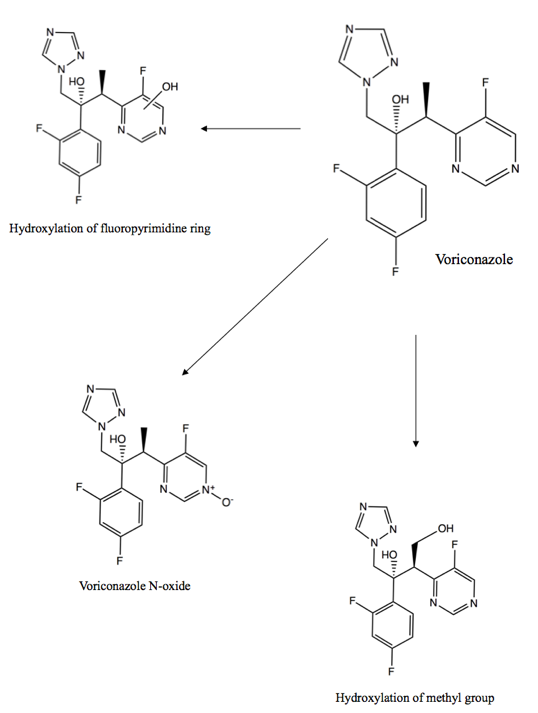
Figure 1. Chemical structures of the main voriconazole metabolites. The three primary routes of voriconazole metabolism are hydroxylation of the fluoropyrimidine ring, hydroxylation of the methyl group, and N-oxidation [Article:12756205]. The notation used with regard to the OH group in the “Hydroxylation of the fluoropyrimidine ring” metabolite indicates that the location of the attachment of the OH group is variable – OH is bonded to the ring, but at an unspecified or unknown atom of the ring.
Pharmacogenetics
Studies on the pharmacogenetics of voriconazole have been done in both healthy adult individuals and immunocompromised patients. Studies on healthy adults measured differences between CYP2C19 genotypes for a variety of pharmacokinetic parameters, such as clearance, area under the plasma concentration-time curve (AUC), median residence time (MRT), maximum plasma concentration (Cmax), trough concentration, and elimination half-life (T1/2) [Articles:16890574, 20002085, 18982321]. For the purposes of this review, we will occasionally group these parameters together and refer to CYP2C19 genotypes as affecting the “metabolism” of voriconazole. Studies in immunocompromised patients focused exclusively on trough or dose-adjusted trough concentrations of voriconazole [Articles:25084200, 26775563, 24403552]. A major limitation of voriconazole pharmacogenetic studies is small cohort sizes – across studies on poor metabolizers (PMs), intermediate metabolizers (IMs) and ultrarapid metabolizers (UMs), approximately half of all studies had less than 30 individuals, the majority had less than 50, and only two studies included over 100 individuals [Articles:25239277, 26982740]. One meta-analysis has examined the association between CYP2C19 variants and voriconazole trough concentrations and clinical outcomes: Li et al. found that PMs had increased trough concentrations as compared to normal metabolizers (NMs) and IMs across 6 studies, and that IMs had increased trough concentrations as compared to NMs across 7 studies. They also found that PMs had increased treatment success as compared to NMs (across 4 studies); however, no significant association with adverse effects was seen between PMs, IMs, NMs and UMs [Article:27388292]. Literature evidence for the effect of variants in other genes involved in voriconazole metabolism or concentration, such as CYP3A4 and CYP2C9, is very limited. One recent study found that dosing voriconazole based on CYP2C19 genotype leads to faster achievement of target concentrations, suggesting that preemptive CYP2C19 genotyping may be useful in the clinic [Article:26616742].
CYP2C19
Since CYP2C19 is the primary enzyme responsible for the metabolism of voriconazole, almost all pharmacogenetic studies on the drug have focused on the contribution of CYP2C19 genotypes or resulting metabolic phenotypes. The CYP2C19 gene is highly polymorphic, with over 30 known variant alleles (http://www.cypalleles.ki.se/cyp2c19.htm). However, the majority of individuals will carry the *1, *2, *3 or *17 alleles. The CYP2C19*1 allele is associated with a normal-functioning CYP2C19 enzyme, while CYP2C19*2 (rs4244285; 19154G>A) and *3 (rs4986893; 17948G>A) are the most common alleles associated with enzymatic loss-of-function [Article:22027650]. The *2 allele varies in frequency between populations, with frequencies of approximately 15% in Caucasians, 18% in African Americans and 29-34% in Asians. The *3 allele is much rarer, with frequencies of approximately 0.6% in Caucasians, 0.3% in African Americans, and 2-9% in Asians. Other alleles have also been associated with significantly decreased or no function (e.g. *4-*10), but they are very rare, with frequencies typically below 1% across ethnicities [Articles:25974703, 22027650]. Additionally, their functional status with specific regard to voriconazole has not been studied. The CYP2C19*17 allele (rs12248560; -806C>T) results in increased activity of the enzyme, with frequencies of approximately 22% in Caucasians, 19% in African Americans, 2% in East Asians and 17% in South or Central Asians [Article:22027650]. For more information on CYP2C19 alleles, their functionality and their population frequencies, please refer to the gene-specific information table page for CYP2C19.
Based on presence of these alleles, individuals can be categorized as CYP2C19 ultrarapid metabolizers (UM), normal metabolizers (NM), intermediate metabolizers (IM; also referred to as heterozygous extensive metabolizers (HEM)) or poor metabolizers (PM). Individuals who are NMs are homozygous for the CYP2C19*1 allele and have a normally functioning enzyme. Those who are IMs carry one *1 allele and a loss-of-function allele (e.g. *1/*2), which produces an enzyme with reduced function. PMs carry two loss-of-function alleles (e.g. *2/*2), resulting in low or deficient CYP2C19 enzyme activity. UMs carry the *17 allele without a loss-of-function allele (i.e. *1/*17 or *17/*17), resulting in increased CYP2C19 enzyme activity [Article:22027650]. Though most studies have categorized *1/*17 as an ultrarapid metabolizer [Articles:26239729, 25239277], it is occasionally grouped with the normal metabolizer phenotype [Article:24475354]. Individuals who carry a loss-of-function allele and a gain-of-function allele (e.g. *2/*17) are typically classified as IMs [Articles:25974703, 23698643].
Poor metabolizers
Across 17 studies and a meta-analysis, poor metabolizers were consistently found to have reduced metabolism leading to increased concentrations of voriconazole as compared to NMs [Articles:15179414, 16890574, 19033450, 18982321, 19299322, 20002085, 20669013, 21383338, 25999694, 21615537, 23400848, 24403552, 25239277, 26024717, 23588332, 25084200, 25451051, 27388292]; one study and a meta-analysis found that PMs had reduced metabolism as compared to IMs [Articles:20669013, 27388292]. However, very little evidence exists for an effect of PM genotypes on clinical outcome. One case report noted a patient with the *2/*2 genotype who discontinued voriconazole due to highly elevated levels [Article:21615537]. Another case report on an individual with the *2/*2 genotype noted that the drug was discontinued due to QTc prolongation occurring while the drug was at toxic levels. However, the study stated that the QTc prolongation might have been due to other causes, such as electrolyte abnormalities [Article:23400848]. A larger study on pediatric patients reported one PM patient with high voriconazole levels who developed syndrome of inappropriate antidiuretic hormone secretion (SIADH) and discontinued the drug [Article:23588332]. Several studies have found no statistically significant difference in the occurrence of drug toxicities (e.g. hepatotoxicity, gastrointestinal effects, photosensitization) between PMs and other metabolizer phenotypes [Articles:24475354, 19261446, 17827141], including the meta-analysis previously discussed above [Article:27388292].
Intermediate metabolizers
Nine studies report an association between intermediate metabolizers and voriconazole metabolism and concentrations [Articles:20002085, 21383338, 23588332, 25084200, 21038076, 26775563], though several did not conduct statistical analyses [Articles:25999694, 25558073, 25155930]. However, almost every study found that IMs had decreased voriconazole metabolism and increased concentrations as compared to NMs. Two exceptions were a study by Shi et al. that found no significant difference in AUC, half-life or clearance between IMs and NMs [Article:20669013], and a study by Wang et al. that found no significant difference in trough concentrations between IMs and NMs, though they did find a significantly increased ratio of voriconazole trough concentrations to voriconazole N-oxide concentrations in IMs compared to NMs [Article:25239277]; no explanation is provided within these studies regarding the contradictory findings. As with PMs, very little evidence exists for an effect of IM genotypes on clinical outcome. One case report noted an individual with the *1/*2 genotype who required a dose reduction due to high trough concentrations [Article:25155930], and another case report noted an individual with the *1/*2 genotype who had elevated concentrations accompanied by hallucinations and abnormal liver function tests. The latter patient’s adverse effects resolved after stopping voriconazole treatment, and reintroduction at a lower dose was uncomplicated [Article:21507170]. A study in pediatrics reported one IM patient with liver function abnormality who required a dose reduction [Article:23588332]. As previously stated under the Poor metabolizers section, no additional studies have reported a statistically significant association between CYP2C19 genetic variations and voriconazole-related adverse events. Most reports to date have been of singular patients or case reports.
Ultrarapid metabolizers
Ten studies have looked at the effect of UM genotypes on the metabolism and plasma concentrations of voriconazole [Articles:18982321, 25239277, 25084200, 26775563, 25558073, 26239729, 23215888, 25986028, 25120580, 22122271], with five focusing exclusively on the *1/*17 genotype [Articles:18982321, 25239277, 26239729, 23215888, 25120580]. One study found that those with the *1/*17 genotype had statistically significantly increased clearance as compared to NMs [Article:18982321]. Two additional studies also found that those with the *1/*17 genotype had decreased concentrations of voriconazole as compared to NMs or PMs, but neither conducted statistical analyses [Articles:25239277, 26239719]. Additionally, two case reports noted subtherapeutic or undetectable levels of the drug in those with the *1/*17 genotype [Articles:23215888, 25120580]. However, in one of these reports, a patient with chronic granulomatous disease had complicated results. The patient had exceptionally high voriconazole concentrations upon initial assessment, but subsequent voriconazole concentrations were so low as to be undetectable; the authors suggest this may be the result of CYP450 enzyme downregulation by inflammation [Article:23215888]. In contrast to these reports, a study in pediatric patients by Hicks et al. found no statistically significant difference in voriconazole dose-adjusted trough concentrations between those with the *1/*17 genotype and those with the *1/*1 genotype [Article:25084200].
Literature evidence on the effect of the *17/*17 genotype on voriconazole levels is sparse. However, the same pediatric study by Hicks et al. found that those with the *17/*17 genotype did have statistically significantly lower dose-adjusted trough concentrations of voriconazole as compared to those with the *1/*1 genotype (four patients with this genotype were present in the study) [Article:25084200]. Two case reports support this association, one describing an individual who had undetectable levels of drug, prompting a discontinuation of voriconazole and switch to an alternative drug [Article:22122271], and the other describing an individual with acute leukemia who had a lack of response and a failure to reach therapeutic concentrations, also prompting discontinuation and switch to caspofungin [Article:26138512]. However, in the former case study, the authors noted that the patient was co-medicated with carbamazepine, a known CYP2C19 inducer, and therefore the individual contributions of the genotype and co-medication cannot be distinguished [Article:22122271]. In the latter study, the authors state that co-medications and disease-induced modulation of CYP2C19 and CYP3A4 cannot be excluded as explanations for the low voriconazole concentrations [Article:26138512].
Additionally, one study in lung transplant patients found that those with the *1/*17 or *17/*17 genotypes had a statistically significantly increased risk for squamous cell carcinoma (SCC) when receiving voriconazole [Article:26982740]. SCC can lead to numerous cutaneous lesions, which may require surgery, and in some case, be fatal; voriconazole use is associated with a 73% increased risk of the disease in lung transplant recipients [Article:26372838]. The authors of the study on CYP2C19 UMs and SCC suggest that the increased risk of SCC may be due to a link between the voriconazole N-oxide metabolite and DNA damage [Article:26982740].
Genotype-directed dosing of voriconazole
Lamoureux et al. sought to determine the impact of CYP2C19 genotypes on the dose required to attain therapeutic voriconazole plasma concentrations in a cohort of 35 patients. They found that the therapeutic dose requirement did not differ between NMs and IMs or PMs. However, UMs had a significantly greater dose requirement as compared to NMs, and also showed an approximately 1.5-fold greater dose requirement as compared to IMs or PMs (UMs: 4.76±0.47 mg/kg twice daily vs. IMs/PMs: 3.03±0.36 mg/kg twice daily) [Article:26775563]. A recent study by Teusink et al. compared standard dosing of voriconazole to genotype-directed dosing [Article:26616742]. A pilot study followed 25 individuals undergoing hematopoietic stem cell transplantation (HSCT) who received an initial dose of voriconazole of 5 mg/kg twice daily, regardless of genotype. Their doses were then adjusted until they were within the target therapeutic range of 1 - 5.5 ug/L. A subsequent study genotyped 20 individuals for CYP2C19 *2, *3 and *17 prior to administering voriconazole, and adjusted the initial voriconazole dose based on their genotype as follows: IMs or unknown metabolizers received 6 mg/kg/dose every 12 hours, and NMs or UMs received 7 mg/kg/dose every 12 hours. No PMs were present and only one UM (*1/*17) was present in the genotype-directed dosing arm. Doses were then adjusted, as in the pilot study, until they were within the target range. Comparison of the genotype-directed dosing arm to the standard dosing arm showed that patients in the genotype-directed dosing arm took a median of 6.5 days to reach the target therapeutic range, while patients in the standard dosing arm took a median of 29 days, a statistically significant difference [Article:26616742].
Other genes
While CYP3A4, CYP2C9 and members of the FMO family all contribute to the metabolism of voriconazole, there is very limited evidence for an association between variants within the genes that encode these enzymes and concentrations or pharmacokinetic parameters of voriconazole. One study found that those with the AG genotype at rs4646437 in the CYP3A4 gene had significantly higher concentrations of voriconazole as compared to those with the GG genotype [Article:25515945]. The functional role of the rs4646437 SNP is yet to be determined, but opposing findings have been reported in studies involving tacrolimus, cyclosporine and finasteride - those with the GG genotype were observed to have the highest concentrations of these drugs, followed by the AG genotype and then the AA genotype [Articles:24465960, 25955319]. CYP2C9 also plays a role in voriconazole metabolism, but a single case report on an individual with the *2/*2 (poor metabolizer) genotype found similar pharmacokinetic parameters when compared against healthy volunteers with the *1/*1 genotype [Article:16940139]. To date, there are no studies investigating the effect of FMO family variants on voriconazole metabolism or response.
Conclusions
While a reasonable amount of literature evidence supports an association between CYP2C19 genotype and voriconazole exposure, these supporting studies are mostly underpowered. Larger studies may be necessary to ascertain a more definitive link between the gene and drug. However, feasibility of such large studies can be hindered by the difficulty of finding enough patients who are PMs, IMs or UMs; international collaborations could assist in recruiting patients with diverse CYP2C19 phenotypes. Additionally, findings connecting CYP2C19 polymorphisms to voriconazole clinical outcomes and adverse events have not been consistent. Hence, more studies are needed to address this potential association. While one study did prospectively genotype CYP2C19 and showed a faster achievement of target voriconazole concentrations, this conclusion is limited due to the study’s small size, lack of PMs, and having only a single UM participant in the genotype-directed dosing arm [Article:26616742]. These issues with the current body of literature warrant further research into this topic given the high morbidity and mortality rates of failed antifungal therapy in immunocompromised patients. Recently published guidelines by the Clinical Pharmacogenetics Implementation Consortium (CPIC) [Article:27981572] providing therapeutic recommendations for voriconazole based on CYP2C19 genotype may help clinicians in delivering more accurate dosing, possibly preventing delays in treatment optimization or unwanted adverse events.
Reactions & interactions (19)
-
Biochemical Reaction
voriconazole → 4-hydroxyvoriconazole
-
Biochemical Reaction
voriconazole → voriconazole n-oxide
-
Biochemical Reaction
voriconazole → hydroxyvoriconazole
-
Biochemical Reaction
dihydroxyvoriconazole → dihydroxyvoriconazole o-glucuronide
-
Biochemical Reaction
hydroxyvoriconazole → hydroxyvoriconazole o-glucuronide
-
Biochemical Reaction
hydroxyvoriconazole → dihydroxyvoriconazole
-
Biochemical Reaction
4-hydroxyvoriconazole → 4-hydroxyvoriconazole 4-o-glucuronide
-
Catalysis
CYP3A4 → Biochemical Reaction
-
Catalysis
FMO3 → Biochemical Reaction
-
Catalysis
FMO1 → Biochemical Reaction
-
Catalysis
CYP3A4 → Biochemical Reaction
-
Catalysis
FMO5 → Biochemical Reaction
-
Catalysis
CYP2C9 → Biochemical Reaction
-
Catalysis
CYP2C19 → Biochemical Reaction
-
Catalysis
CYP2C19 → Biochemical Reaction
-
Catalysis
UGT1A4 → Biochemical Reaction
-
Catalysis
UGT1A4 → Biochemical Reaction
-
Catalysis
CYP2C19 → Biochemical Reaction
-
Catalysis
UGT1A4 → Biochemical Reaction
Edit history (3)
- 2016-09-30 Create
- 2022-05-26 Update Added tag for anti-infective agents
- 2024-07-11 Update fixed typo