About this pathway
Background
Pazopanib is a small molecule, orally active anti-cancer drug approved by the US-FDA and the EMA for the treatment of patients with metastatic renal cell carcinoma (RCC) and soft tissue sarcoma [Articles:22341567, 24041629]. It is a second-generation anti-angiogenesis tyrosine kinase inhibitor (TKI) regarded as having a more selective set of target receptors and thus was considered likely to incur fewer side effects than first generation multi-target TKIs for RCC such as sunitinib and sorafenib [Article:18230058].
Pharmacodynamics
Pazopanib is targeted against the vascular endothelial growth factor receptors VEGFRs (coded for by FLT1, KDR and FLT4), platelet derived growth factor receptors PDGFRs (PDGFRA and PDGFRB) and KIT [Articles:17620431, 18230058]. Inhibition of the receptors blocks downstream activation of multiple signaling pathways that contribute to angiogenesis including the RAS/RAF/MEK/ERK, PI3K/AKT/mTOR and IP3 pathways (see VEGF signaling pathway (PA2032) for further discussion of downstream signaling and details of candidate genes).
Pharmacokinetics
There is wide interpatient variability on pazopanib pharmacokinetics, PK [Article:25271729]. There is also considerable intrapatient variability in PK, ie. differences over time in the same patient [Article:25271729]. The sources of these differences may be due to differential absorption, metabolism or elimination: including timing of the interval between food consumption and pazopanib intake, consumption of other drugs or bioactive foods, and the activity or expression of drug transporters and liver enzymes.
Absorption and distribution
Similar to many other oral kinase inhibitors, pazopanib is a biopharmaceutics classification system Class 2 drug (high permeability, low solubility). Pazopanib is soluble at pH 1 and practically insoluble above pH 4 in aqueous media [Article:23636448]. Stomach acid and stomach contents therefore have a significant effect on absorption of pazopanib [Article:23636448]. Administration of oral pazopanib with food in patients with cancer increased the AUC and Cmax twofold with either high-fat or low-fat meals [Article:20980999]. Similarly, crushing pazopanib tablets or giving the drug as an oral suspension increases the rate and extent of oral absorption, with increases in AUC and Cmax and decreased Tmax [Article:21811833]. Esomeprazole (a proton pump inhibitor) reduces exposure of pazopanib by preventing absorption [Article:23636448]. The drug label recommends alternate dosing schedules for patients who require medicines that increase gastric pH.
Both in vitro and in plasma samples from cancer patients, pazopanib is highly bound to protein (greater than 99.9% of drug) [Article:26572909]. Since unbound drug concentrations are thought to be more relevant to kinase inhibition, even small differences in drug binding due to differences in plasma proteins may have effects on kinase inhibition at the site of action. In studies of plasma from volunteers and cancer patients, pazopanib had greatest binding affinity for human serum albumin (ALB) with lesser binding to alpha-1 acid glycoprotein (ORM2) and LDL [Article:26572909]. Variations in serum proteins may account for some of the interindividual and intraindividual differences in pazopanib PK and PD. Elimination occurs primarily via feces and less than 4% is excreted in urine.
Metabolism
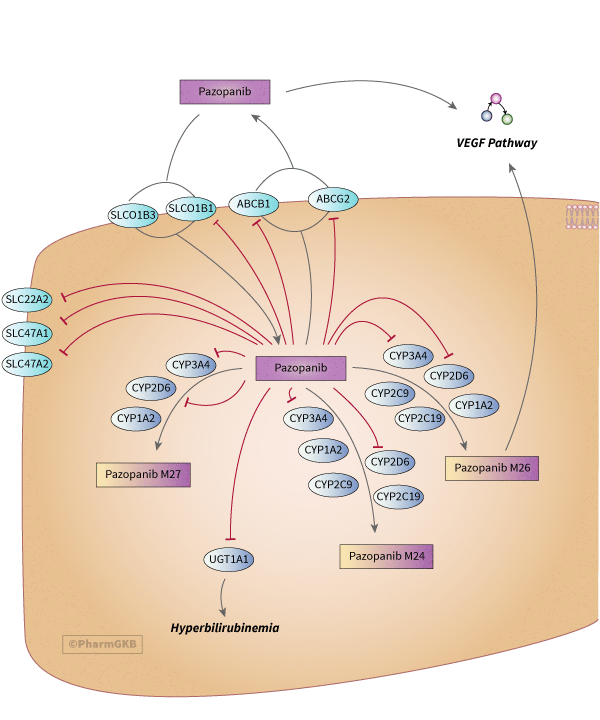
Pazopanib is primarily metabolized by CYP3A4 and to a lesser extent by CYP1A2 [Articles:23636448, 20881954]. Some reviews also list CYP2C8 as important and reference the drug label, but direct evidence in the literature is lacking. Early PK was reported in documents submitted to the FDA detailing experiments in microsomes, human hepatocytes, animal models and human plasma from a phase I clinical trial in patients with solid tumors FDA link. The metabolites M24 and M26 were detected from microsomes expressing CYP1A2, CYP2C9, CYP2C19, CYP2D6, and CYP3A4; M27 was detected from microsomes with CYP1A2, CYP2D6, and CYP3A4; and M12 and M16 were only detected with CYP3A4 microsomes FDA doc page 143. In plasma, the main products identified on Day 22 were mono-oxygenated products M24 (approximately 11%); demethylated products M26 (6.5%), M27 (3%) and M28 (1%); and unchanged parent compound FDA doc page 129. The most commonly discussed metabolites in the peer-reviewed literature are M24 (GSK1268992, CID 72942037), M26 (GSK1268997, CID 72942038) and M27 (GSK1071306, CID 68319455) [Article:23636448]. When CYP3A4 is inhibited by ketoconazole, there is a reduction in metabolites M26 and M27 but not M24 exposure, suggesting that the relative formation of metabolites by each CYP is not equivalent [Article:23636448]. While M26 demonstrated potency similar to that of pazopanib in vitro in HUVEC cells, other metabolites were 10- to 20- fold less active documents submitted to Australian Dept of Health.
There is a complex relationship between pazopanib and the enzymes and transporter that it interacts with. In addition to being metabolized by CYP3A4, pazopanib also inhibits CYP3A4 [Article:24713129]. In a phase 1 study of pazopanib plus paclitaxel (which is also metabolized by CYP3A4 and by CYP2C8), authors observed an approximately 40% increase in paclitaxel exposure whereas pazopanib exposure was not related to paclitaxel dose [Article:25504632]. Furthermore, in the same study of pazopanib plus paclitaxel, one patient who was taking simvastatin (mostly metabolized by CYP3A4 with some involvement of CYP2C8) and had reduced activity of CYP2C8 (CYP2C8*3*3) experienced hepatotoxicity that resolved after simvastatin was withdrawn [Article:25504632]. This suggests that the hepatotoxicity was most likely related to altered simvastatin metabolism, and that when there is competition for CYP3A4 and CYP2C8 pazopanib metabolism is favored over either paclitaxel or simvastatin. However, this is not the case with all drug combinations. The pazopanib drug label recommends avoidance of strong inhibitors of CYP3A4 (such as ketoconazole and grapefruit juice) that may increase plasma pazopanib concentrations, and strong inducers of CYP3A4 (such as rifampin) that may reduce plasma concentration of pazopanib. Pazopanib is also a weak inhibitor of CYP2D6 as reported in drug label and supported by published studies examining the effects of various probe drugs in cancer patients [Article:20881954].
Pazopanib is an inhibitor of UGT1A1 FDA drug label. It is not discussed whether pazopanib or its metabolites are also substrates of UGT1A1, although glucuronidated products are mentioned as being produced by human hepatocytes in the FDA documentation (page 144). The drug label has warnings for individuals with Gilbert’s syndrome (UGT1A1 *28/*28 genotype), where the activity of UGT1A1 is impaired and there is a greater risk for hyperbilirubinemia (see PGx section below for details of published studies supporting this).
Transport
Pazopanib is a substrate for efflux transporters ABCB1 (also known as PgP and MDR1) and ABCG2 (also called BCRP) [Articles:27418107, 22918879, 22688250]. Studies in transfected cell lines suggest that pazopanib is a weak substrate for ABCB1 and a stronger substrate for ABCG2 but both were equally important for transport at the blood-brain barrier in a mouse model study [Article:22688250]. Several TKIs are able to act as both substrate and inhibitors for ABCB1 and ABCG2, and in vitro studies indicate that pazopanib is a strong inhibitor of both transporters [Article:27418107]. The pazopanib drug label also indicates that it is an inhibitor of ABCB1.
Pazopanib is an inhibitor of OCT2 (SLC22A2), MATE1 (SLC47A1) and MATE2-K (SLC47A2) renal transporters. This inhibition results in a decrease of cisplatin uptake by these transporters and attenuates cisplatin-induced cytotoxicity in vitro. [Article:27178732]. The relationship of pazopanib with organic anion transporting peptides appears contradictory: In studies of transfected HEK293 cells cellular uptake of pazopanib was facilitated by both OATP1B1 (SLCO1B1) and OATP1B3 (SLCO1B3) [Article:23340295]. Whereas in transfected CHO cells, pazopanib was shown to be an inhibitor of OATP1B1 (SLCO1B1) but not OATP1B3 (SLCO1B3) [Article:24807167] and other studies in CHO cells concluded that pazopanib did not exhibit any substrate specificity toward OATP1B1 and OATP1B3 [Article:24643910].
Pharmacogenomics
There are relationships between pazopanib exposure and both efficacy and toxicity, suggesting that pharmacogenomics variants that alter pazopanib exposure could be clinically relevant. Specifically, Suttle and colleagues demonstrated an association between pazopanib steady-state trough concentration (with a steady state threshold concentration of 20.5 µg/mL) and clinical response, as measured by PFS or tumor shrinkage. They also found strong correlations between trough concentrations and drug-related adverse events, such as increased blood pressure and hand-foot syndrome [Article:25349968]. A recent paper suggests that hypertension is not itself significantly related to overall survival and that treating this side effect should not compromise efficacy [Article:26702763]
Toxicity PGx
Adverse events associated with pazopanib treatment are diarrhea, hypertension, nausea, anorexia, vomiting, hair color changes, increase in alanine transferase or aspartate aminotransferase levels, hyperglycemia, leucopenia, neutropenia and hyperbilirubinemia [Article:22733795].
Although CYP3A4 is the major metabolizing enzyme of pazopanib, CYP3A4 polymorphisms have no known effect on pazopanib pharmacokinetics [Article:22733795]. Given the abundance of CYP3A4 relative to other CYPs, and the lack of a null allele [Article:12406645], it is not surprising that there is no strong effect of CYP3A4 variants on pazopanib PGx. There are other PK related gene variants associated with pazopanib toxicity, as shown in table 1a, in addition to variants in genes involved in liver function and in pazopanib PD.
There is evidence that transporter variants, specifically in ABCG2, can impact pazopanib toxicity. In a phase 1 study of patients with advanced solid tumors receiving pazopanib (n=28), one patient homozygous for the reduced activity variant ABCG2 *2 (rs2231142 TT genotype) discontinued treatment due to grade 3 hepatotoxicity [Article:25504632]. Additionally, in retrospective analysis of clinical trial data, individuals who were carriers of the T allele of ABCG2 rs2231142 were more likely to experience elevations in alanine aminotransferase (ALT greater than 3 × ULN) when treated with pazopanib and simvastatin as compared to those with the GG genotype. However, the number of patients on both drugs was small (n=41) [Article:22918879]. This polymorphism was not associated with ALT elevations in pazopanib-treated patients without concurrent use of statins (n=895) or taking other statins [Article:22918879]. However the allele frequencies in this population were not described. The frequency of the ABCG2 rs2231142 allele varies from rare in Black or African American populations (1-5%), to around 10% in White populations, to 30-35% in Asian populations Hapmap3. It is possible that the homozygous minor allele could still be a risk factor even in the absence of simvastatin but was not found at a high enough frequency in the population tested.
Studies have revealed an association between pazopanib treatment and UGT1A1 polymorphisms. Certain UGT1A1 polymorphisms are associated with mildly dysfunctional bilirubin metabolism in the absence of drug. When UGT1A1 is inhibited by pazopanib this exacerbates the phenotype leading to hyperbilirubinemia. In a study consisting of 116 patients in Phase 2 and 130 patients in Phase 3 with advanced RCC undergoing pazopanib treatment, UGT1A1*28 (rs8175347) homozygotes and heterozygotes had increased bilirubin levels [Article:20389299]. Other UGT1A1 polymorphisms like UGT1A1*36, *37 and *6 alleles also decrease UGT1A1 activity/expression. In another Phase 3 study of advanced patients with RCC, UGT1A1*36, *37 and *6 alleles were associated with hyperbilirubinemia [Article:24107802].
Variants in the HFE gene (rs2858996 and rs707889) have been shown to be associated with elevated ALT in RCC patients treated with pazopanib [Article:21145803]. The functional relevance of the SNPs is unknown with the authors stating they found no noteworthy in silico predictions. The HFE variants may have a subtle phenotype of chronic iron deposition and associated oxidative stress that in the presence of pazopanib may put patients at greater susceptibility to cellular injury and resultant ALT elevations. Alternatively the HFE gene is located in a region of chromosome 6 that contains the HLA genes, several of which are associated with drug-induced liver injury [Articles:21145803, 25491399].
While the VEGFA gene is part of the PD pathway, and thought of more in terms of effects on efficacy, its variants have also been associated with toxicity. A small phase 1 study of pazopanib and pemetrexed in patients with solid tumors (n=16) found that those with the C allele of rs833061 in VEGFA were more likely to experience severe neutropenia than TT homozygotes [Article:23179337].
Efficacy PGx
Several polymorphisms in genes directly involved in pazopanib pharmacodynamics have been reported: KDR (target), VEGFA (endogenous ligand for target) in addition to variants in genes that are involved in inflammation (e.g. CXCL8) and transcriptional regulation (HIF1A and NR1I2).
In a study of 397 patients with metastatic RCC treated with pazpanib, three VEGFA promoter alleles (-1498 rs833061 C allele, -2578 rs699947 A and -634 rs2010963 G) were associated with decreased response rate [Article:21576632]. These were confirmed in a small study of 19 patients with RCC to be associated with PFS [Article:27175586]. Interestingly this small study found the effects of these VEGFA variants to be the opposite in PFS of patients treated with sunitinib [Article:27175586].
Maitland and colleagues identified a variant (rs34231037) in KDR, the gene that encodes VEGFR2, that is a significant predictor of soluble VEGFR2 concentrations in healthy individuals and cancer patients treated with pazopanib [Article:25411163]. This variant was also correlated with response to pazopanib.
IL-8 (coded for by the CXCL8 gene) is a chemokine that triggers inflammatory processes such as migration of neutrophils, monocytes and endothelial cells and promotes angiogenesis [Articles:18579287, 26893688]. The A allele of a promoter variant in CXCL8 rs4073, is associated with increased IL-8 production in response to inflammatory stimuli such as respiratory syncytial virus [Article:15085176], Acute Respiratory Distress Syndrome [Article:17498967] and increased risk for certain cancers [Articles:24760271, 26885219]. The rs4073 (-251) AA genotype was associated with decreased PFS in RCC [Article:21576632]. The rs4073 A allele was associated with decreased overall survival when treated with pazopanib or sunitinib in patients with RCC as compared to the T allele and this was confirmed in a meta-analysis [Article:25695485]. CXCL8 rs1126647 (2767) is linked in haplotype with rs4073 and associated with Age-related macular degeneration, an angiogenesis-related disease [Article:23840568]. The T allele of rs1126647 is associated with decreased PFS, OS and response rate in studies and meta-analyses of RCC patients treated with pazopanib [Articles:21576632, 25695485].
Conclusions
There is evidence of relationships between pazopanib efficacy and/or toxicity and genes in the pharmacokinetic and/or pharmacodynamic pathways. Further confirmation is needed for the PGx candidate variants in ABCG2, UGT1A1, VEGFA and CXCL8 in particular. More studies are needed in diverse groups where transporter variants are present at different frequencies to better predict toxicity Pending validation these candidate PGx variants have great potential for clinical relevance in preventing toxicity, guiding TKI choice and improving efficacy.
Reactions & interactions (45)
-
Biochemical Reaction
pazopanib → pazopanib M26
-
Biochemical Reaction
pazopanib → pazopanib M24
-
Biochemical Reaction
pazopanib → pazopanib M27
-
Catalysis
ABCG2 → Transport
-
Catalysis
ABCB1 → Transport
-
Catalysis
SLCO1B1 → Transport
-
Catalysis
SLCO1B3 → Transport
-
Catalysis
CYP3A4 → Biochemical Reaction
-
Catalysis
CYP1A2 → Biochemical Reaction
-
Catalysis
CYP2D6 → Biochemical Reaction
-
Catalysis
CYP2C9 → Biochemical Reaction
-
Catalysis
CYP2C19 → Biochemical Reaction
-
Catalysis
CYP3A4 → Biochemical Reaction
-
Catalysis
CYP2D6 → Biochemical Reaction
-
Catalysis
CYP1A2 → Biochemical Reaction
-
Catalysis
CYP2C9 → Biochemical Reaction
-
Catalysis
CYP2C19 → Biochemical Reaction
-
Catalysis
CYP2D6 → Biochemical Reaction
-
Catalysis
CYP1A2 → Biochemical Reaction
-
Catalysis
CYP3A4 → Biochemical Reaction
-
Inhibition
pazopanib → KIT
-
Inhibition
pazopanib → ABCG2
-
Inhibition
pazopanib → FLT4
-
Inhibition
pazopanib → PDGFRA
-
Inhibition
pazopanib → SLCO1B1
-
Inhibition
pazopanib → CYP2D6
-
Inhibition
pazopanib → UGT1A1
-
Inhibition
pazopanib → SLC47A1
-
Inhibition
pazopanib → CYP3A4
-
Inhibition
pazopanib → KDR
-
Inhibition
pazopanib → PDGFRB
-
Inhibition
pazopanib → FLT1
-
Inhibition
pazopanib → ABCB1
-
Inhibition
pazopanib → SLC47A2
-
Inhibition
pazopanib → SLC22A2
-
Leads To
KDR → VEGF Signaling Pathway
-
Leads To
pazopanib M26 → VEGF Signaling Pathway
-
Leads To
UGT1A1 → Hyperbilirubinemia
-
Leads To
FLT1 → VEGF Signaling Pathway
-
Leads To
FLT4 → VEGF Signaling Pathway
-
Leads To
PDGFRA → VEGF Signaling Pathway
-
Leads To
KIT → VEGF Signaling Pathway
-
Leads To
PDGFRB → VEGF Signaling Pathway
-
Transport
pazopanib → pazopanib
-
Transport
pazopanib → pazopanib
Edit history (3)
- 2017-03-16 Create
- 2018-09-07 Update Updated image files for formatting.
- 2022-09-23 Update fixed typos