About this pathway
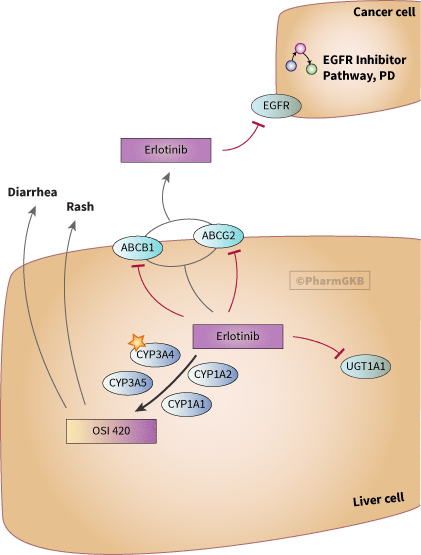
Erlotinib hydrochloride (Tarceva, OSI-774, CP-358774) is a small molecule, orally active anilinoquinazoline compound that reversibly and selectively binds to the ATP-binding site of epidermal growth factor receptor (EGFR). This prevents autophosphorylation of tyrosine residues associated with EGFR, thereby inhibiting further downstream signaling [Articles:14676101, 15217965].
After oral administration erlotinib is widely distributed throughout the body. Its primary method of elimination is by biotransformation to a pharmacologically active O-desmethyl metabolite, OSI-420. Erlotinib is metabolized in the liver by mainly by CYP3A4, with contributions from CYP3A5, CYP1A2 and CYP1A1 [Article:24781527]. Extra-hepatic metabolism is mediated by CYP3A4 in the intestine, CYP1A1 in lungs, and CYP1B1 in tumor tissue [Articles:17575239, 25027951]. Erlotinib also inhibits ATP-binding cassette (ABC) efflux transporters like ABCB1/MDR1 and breast cancer resistance protein (ABCG2/BCRP1)) via direct inhibition of the drug efflux function of MDR1 and BCRP1 (PMID: 18006847). In addition, erlotnib is also a potent inhibitor of UGT1A1 in vitro [Article:19850672]. UDP-glucuronosyltransferases (UGTs) catalyze glucuronidation of approximately 35% of all drugs metabolized by phase II enzymes. Thus, erlotinib might also alter exposure of co-administered drugs that are substrates of these enzymes.
There is wide inter-individual variability (up to 7 fold) in erlotinib exposure. In addition, difference in pharmacokinetics of erlotinib and OSI-420 was observed in smokers and non-smokers [Article:16609030]. This may be due to induction of CYPA1/A2 by cigarette smoke, consequently decreasing erlotinib by 50-60% [Article:18000659]. Skin toxicity and diarrhea are common adverse events associated with erlotinib treatment [Article:15310767]. Severity of skin rash may be a surrogate marker for favorable response. In BR21 study, strong correlation was observed between higher-grade 2 skin rash and improved overall survival in patients with non-small cell lung cancer undergoing erlotinib treatment when compared to those without skin rash (P<0.001)[Article:17606725]. In another study of 46 patients with stage IV non-small cell lung cancer, patients with grade 3 skin toxicity were associated with higher levels of erlotinib in serum after 7 days of treatment along with longer progression-free (P=0.009) and overall survival (P=0.006) when compared to those with grade 0-2 skin toxicities [Article:24388705].
Pharmacogenetic changes have also been implicated in erlotinib-mediated adverse events. In a study of 50 Japanese patients, there was a statistically significant association between patients with ABCB1 1236C>T (rs1128503)-2677G>T (rs2032582)-3435C>T (rs1045642) genotypes (n=6) and cumulative incidence of grade 2 or higher toxicity (skin rash or diarrhea) when compared to patients with wildtype genotypes (n=44, P=0.012)[Article:22462752]. Due to small sample size, further studies are required to confirm the effect of ABCB1 polymorphisms on erlotinib-dependent toxicity.
Genetic polymorphisms in enzyme and transporters involved in pharmacokinetics of erlotinib may affect its exposure, although the effect appears to be small [Article:21553932]. In a study of 80 cancer patients receiving 150mg/day erlotinib, there was no statistically significant effect of CYP3A4/3A5 on erlotinib pharmacokinetics [Article:18309947]. Patients homozygous for CYP3A4*1B (low expressor) and CYP3A4*3 (non-expressor) were associated with 21% higher AUC (P=0.090) and 26% higher trough plasma concentration (P=0.079) than those with other diplotypes, although this change was not statistically significant. Additionally, polymorphisms in ABCG2 promoter involving -15622C/T (rs7699188) and 1143C/T (rs2622604) were associated with statistically significant higher AUC (P<0.05) and trough plasma concentration (P<0.05).
Reactions & interactions (14)
-
Biochemical Reaction
erlotinib → osi 420
-
Catalysis
ABCB1 → Transport
-
Catalysis
ABCG2 → Transport
-
Catalysis
CYP3A4 → Biochemical Reaction
-
Catalysis
CYP1A1 → Biochemical Reaction
-
Catalysis
CYP3A5 → Biochemical Reaction
-
Catalysis
CYP1A2 → Biochemical Reaction
-
Inhibition
erlotinib → EGFR
-
Inhibition
erlotinib → UGT1A1
-
Inhibition
erlotinib → ABCG2
-
Inhibition
erlotinib → ABCB1
-
Leads To
osi 420 → Exanthema
-
Leads To
osi 420 → Diarrhea
-
Transport
erlotinib → erlotinib
Edit history (5)
- 2008-12-02 Create
- 2012-06-04 Update
- 2019-03-06 Update Updated to new illustrator formatting.
- 2019-03-06 Update Updated text to include more references.
- 2019-03-06 Update Updated gpml. Removed CYP2C8 due to lack of evidence.